PHTY208 Lecture Notes - Lecture 12: Basophil, Catecholamine, Metabolic Acidosis


Cardiac Pharmacology
• Introduction
o Correct cardiac function depends on
o Adequate amounts of ATP
• Maintain electrochemical gradients
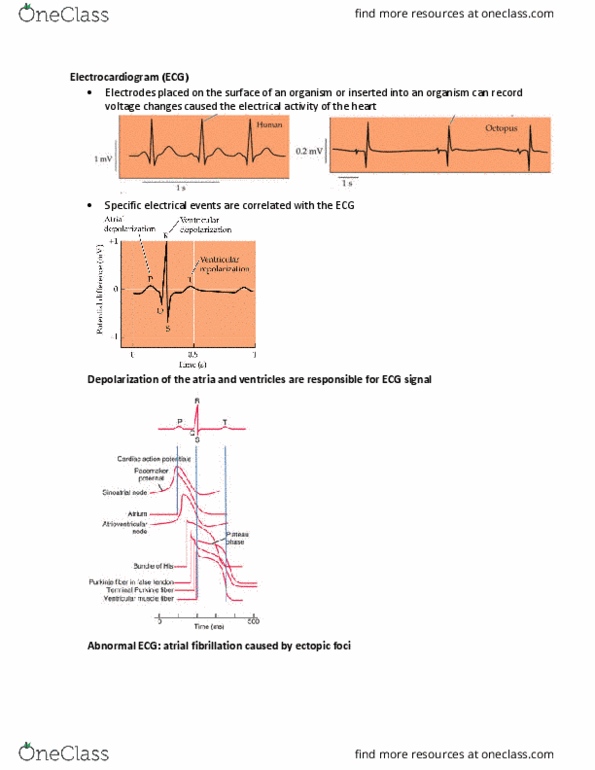
• Propagate action potentials
• Power muscle contraction
o Adequate amounts of Ca++
• Caliu is glue that liks eletrial ad mechanical events
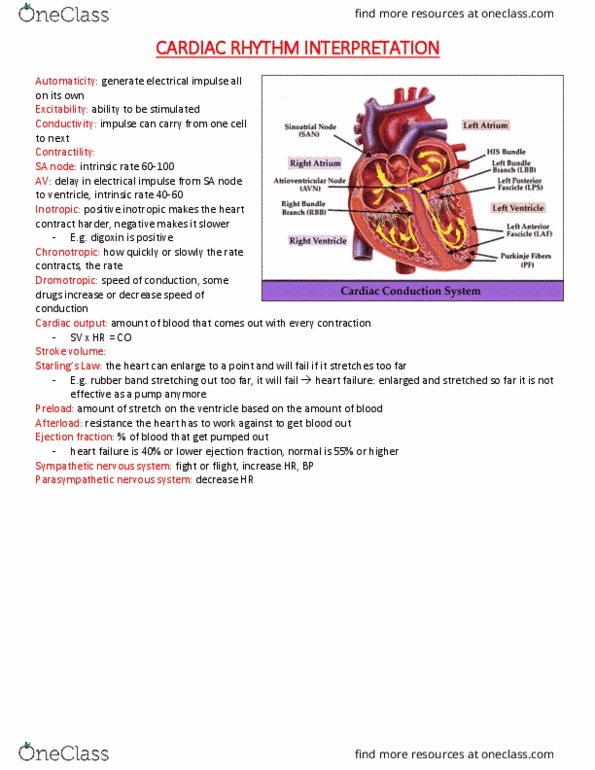
o Coordinated electrical stimulus
• Inotropic drugs and vasopressors
o Drugs affecting cardiac function
• Positive inotropic effect
▪ Increases force of myocardial contraction
• Negative inotropic effect
▪ Decreases force of myocardial contraction
• Positive chronotropic effect
▪ Accelerate the HR by increasing impulses from SA node
• Negative chronotropic effect
▪ Slows the HR by decreasing impulses from SA node
• Positive dromotropic effect
▪ Increase conduction velocity
• Negative dromotropic effect
▪ Decrease conduction velocity
o Inotropic drugs
• Used to increase the force of ventricular contraction
▪ When myocardial systolic function is impaired
• Drugs in this category include
▪ Cardiac glycosides
• Digoxin
• Two effects
• Improve contractility of failing heart
• Prolong refractory period
• Mechanical effect (positive inotropy)
• Inhibits the sarcolemmal Na+/K+ ATPase pump
• Leads to increased calcium in the sarcoplasmic
reticulum
• Electrical effect (negative chronotropy)
• Modifies autonomic nervous system activity,
increasing vagal tone and decreasing sympathetic
activity
• Decreases AV nodal conduction velocity, and
enhances the refractory period, therefore reducing
transmission of atrial impulses to the ventricles
• Clinical uses
• Congestive heart failure – useful in systolic heart
failure
• Augments contractility
find more resources at oneclass.com
find more resources at oneclass.com

• Shown to NOT affect mortality in congestive
heart failure, although it does improve
symptoms
• Tachydysrhythmias
• Reducing the number of impulses transmitted
through the AV node
• Effective rate control of atrial fibrillation and
atrial flutter
• Slowing AV nodal impulse conduction and
increasing the refractory period
• Side effects
• Cardiac: enhances cellular automaticity, and
formation and propagation of impulses
• Also enhances vagal tone – variable degrees of AV
block
• Systemic: nausea, vomiting, anorexia (affects the
medulla); fatigue, weakness
• Visual disturbances, confusion, nightmares, agitation
and drowsiness
▪ Sympathomimetic
• Increase intracellular calcium influx
• Enhances the force of contraction
• Commonly used for heart failure
• Dopamine, dobutamine, norepinephrine, epinephrine
• Clinical effect of dopamine (depends on dose)
• Local vasodilation, increases renal blood flow
• Increase heart rate, cardiac contractility and SV
• Peripheral vasoconstriction (high dose)
• Side effects – acceleration of the heart, tachyarrhythmias
and hypertension
• Positive inotropic effect
• Enhanced entry of calcium into cell – enhanced contraction
• Vasodilation
• Used to treat acute heart failure
• Side effects include
• Provocation of ventricular arrhythmias
• Increased mortality (with chronic use)
• Nausea, vomiting
▪ Phosphodiesterase-3 inhibitors
o Vasopressin
• Endogenous antidiuretic hormone
• Functions to maintain water balance
• Potent vasoconstrictor when IV administered at high dose
• Clinical use
▪ Maintaining blood pressure in patients with vasodilatory shock
▪ Beneficial during cardiac arrest
• Vasodilator drugs
o Play a central role in heart failure and hypertension
o Include
• ACE inhibitors
▪ Block the angiotensin converting enzyme
find more resources at oneclass.com
find more resources at oneclass.com

• Angiotensin II causes vasoconstriction and aldosterone release
• ACE also intactivates bradykinin, a potent vasodilator
▪ Clinical Uses
• Hypertension
• Congestive heart failure
• Ischemic heart disease
▪ Side Effects
• Hypotension – rare
• Hyperkalemia
• Renal insufficiency
• Bilateral renal artery stenosis
• Dry cough – 15% of patients
• Angiotensin II receptor antagonists
▪ Produce vasodilation, naturesis and hypotension
▪ More complete angiotensin blockade than ACE-inhibitors
▪ Clinical uses
• Limited evidence for long term mortality benefit
• Hypertension – similar efficacy to ACE-inhibitors
• Congestive heart failure –as effective as ACE-inhibitors
• Ischemic heart disease – little evidence
▪ Side Effects
• Hypotension – as for ACE-inhibitors
• Hyperkalemia – as for ACE-inhibitors
• Generally well tolerated, no dry cough
• Used in patients unable to tolerate an ACE-inhibitor
• Vasodilators
▪ Potassium channel activators
• Reducing the sensitivity of smooth muscle cells in the walls of
arteries to the normal stimuli to contract
• Widening of the arteries improving the blood supply to the heart
muscle in angina pectoris
▪ Indirect vasodilators
• Inhibit vasoconstriction through mediation of sympathetic
nervous system and inhibitors of RAAS
• Centrally acting adrenergic inhibitors
• Calcium channel blockers (also antiarrhythmics)
• Nitrates
▪ Clinical use – angina, acute ischaemic syndromes in heart failure
▪ At low doses
• Produce preferential venous dilation
• Lowering ventricular wall stress and myocardial oxygen demand
• Also some mild arterial dilation occurs
▪ At higher doses
• Arteriolar dilation -> lowering of blood pressure
• Acute CHF – relieves pulmonary oedema
▪ Side Effects - Hypotension, reflex tachycardia, headache and flushing
• Natriuretic peptides
• Phosphodiesterase-3 inhibitors
• Other drugs acting on RAAS
▪ Renin inhibitors
• That are used primarily in treatment of hypertension.
find more resources at oneclass.com
find more resources at oneclass.com