PHTY211 Lecture Notes - Lecture 7: Casp, Statistical Hypothesis Testing, Straight Leg Raise


Appraising a diagnostic study
• What is a diagnostic study
• Describe what is meant by the terms reference standard, blinded comparison and
diagnostic uncertainty.
• Explain the reasons why use of an adequate reference standard, blinded comparison and
diagnostic uncertainty are important when appraising evidence about diagnosis
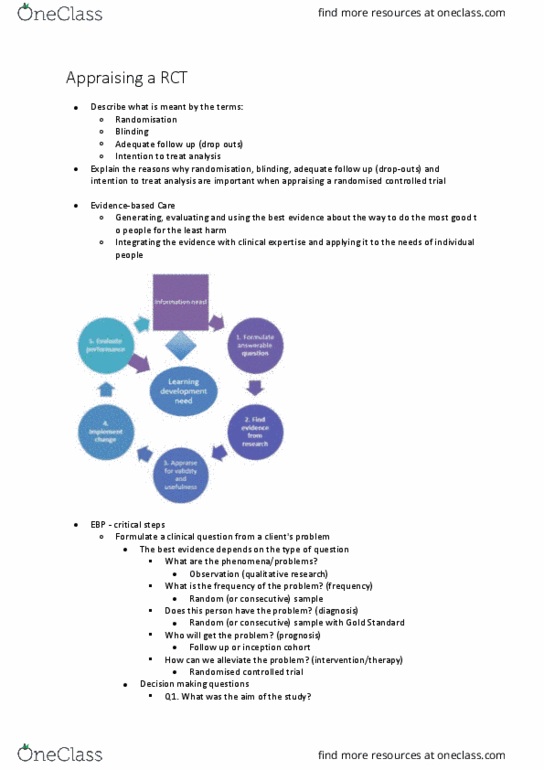
• EBP‐ itial steps
o Foulate a liial uestio fo a liet’s pole
• Refining the question
▪ Patient
▪ Test
▪ Diagnosis
• How accurate is a diagnostic test?
▪ In patients with shoulder pain, how valid are the empty/full can tests in
diagnosing a rotator cuff tear?
▪ What is the auay of the Laha’s test i diagosig ateio
cruciate ligament laxity in athletes with knee pain?
▪ Ca a egatie Phale’s test ule out apal tuel syndrome in
pregnant women?
▪ In patients with acute low back pain, how accurate is the straight leg
raise test in diagnosing a nerve root compromise?
o Search the literature for relevant evidence
• What is the evidence?
▪ Evidence about diagnosis can come from several sources
• Clinical observation
• Apply test to ay people ad see ho ell the test’s
findings correspond with the subsequent correct diagnosis
• Difficult to obtain unbiased estimates in the course of
routine clinical practice
• May be confirmed by subsequent investigations e.g. MRI,
arthroscopy
• Not routinely available
• Accuracy of diagnostic test may be poor estimate
• Clinical research
• Cross sectional studies
• How accurately a test can determine whether a
disease or condition is present at the time the test is
conducted
• Group of subjects subjected to a clinical test of
interest AND results compared to another usually
more invasive test
• Gold standard or reference standard test
• Reference standard may be hindsight as true
diagnosis becomes apparent with time
▪ Coss‐setioal studies
▪ Randomised trials
▪ Screening
• Systematic reviews
• Finding the evidence
find more resources at oneclass.com
find more resources at oneclass.com

▪ Difficult to find
• Relatively few studies
▪ No databases dedicated to archiving studies of diagnosis in
physiotherapy
• General databases
• MEDLINE, Embase, CINAHL, PsycINFO
• Clinical queries
▪ Systematic reviews
• Cochrane library
• Pedro
o Evaluate or critically appraise the evidence for its validity and utility
• Are the study results valid? (internal validity)
▪ Was there comparison with an adequate reference standard?
• Were the findings of the test compared with the findings of a
efeee stadad that is osideed to hae ea‐pefet
accuracy?
• Adequacy of reference standard
• Is it more or less perfectly accurate?
• If imperfect
• Accuracy of diagnostic test of interest will be
underestimated
▪ Was the comparison blind?
• Bias a aise siilaly to RCT’s
• Assessor bias
• Bias estimates of diagnostic accuracy
• Ensure assessor is unaware of findings of both tests
• Confirmation of independence of the tests implies that estimates
of diagnostic accuracy were probably not distorted by assessor
bias
• Better if diagnostic test recorded prior to reference standard
• Were the clinicians who applied the clinical tests unaware of the
findings of the reference standard?
▪ Did the study sample consist of participants for whom there was
diagnostic uncertainty?
• This criterion best discriminates between biased and unbiased
studies of diagnostic test accuracy
• Cohort design
• Tests from sample we would usually test in clinical practice
• Therefore only test those where the diagnosis is suspected
• Provides us with best estimates of diagnostic test accuracy
• Case control design
• Recruits samples who clearly do or do not have diagnosis
• Easier to obtain adequate number of participants with and
without diagnosis
• Methodological cost – diagnostic test is subject to relatively
gentle scrutiny
• Only discriminates between who does and who does not
have diagnosis not making an accurate diagnosis if
suspected of having a diagnosis
• More prone to bias
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Finding the evidence: difficult to find, relatively few studies, no databases dedicated to archiving studies of diagnosis in physiotherapy, general databases, medline, embase, cinahl, psycinfo, clinical queries. False negative: test is negative but do have the condition. False positive: test is positive but don"t have condition, accuracy of diagnostic tests most commonly described in terms of. Sensitivity (snout: proportion (%) who truly have condition and test +ve, helps rule out disease (when the result is negative, out or snout. Specificity (spin: p(cid:396)opo(cid:396)tio(cid:374) (cid:894)%(cid:895) (cid:449)ho t(cid:396)uly do(cid:374)"t ha(cid:448)e (cid:272)o(cid:374)ditio(cid:374) a(cid:374)d test ve, rules in disease with a high degree of confidence. In or spin: desirable to be close to 100% Lr+ = sensitivity/ (100 specificity: values should be >1, useful if >3, very useful if >10, negative, how much more likely a negative test finding is in people who have the condition than in those who do(cid:374)"t.