CAM202 Lecture Notes - Lecture 8: Aluminium Hydroxide, Peptic Ulcer, Gastric Mucosa

11 Oct 2018
School
Department
Course
Professor
Document Summary
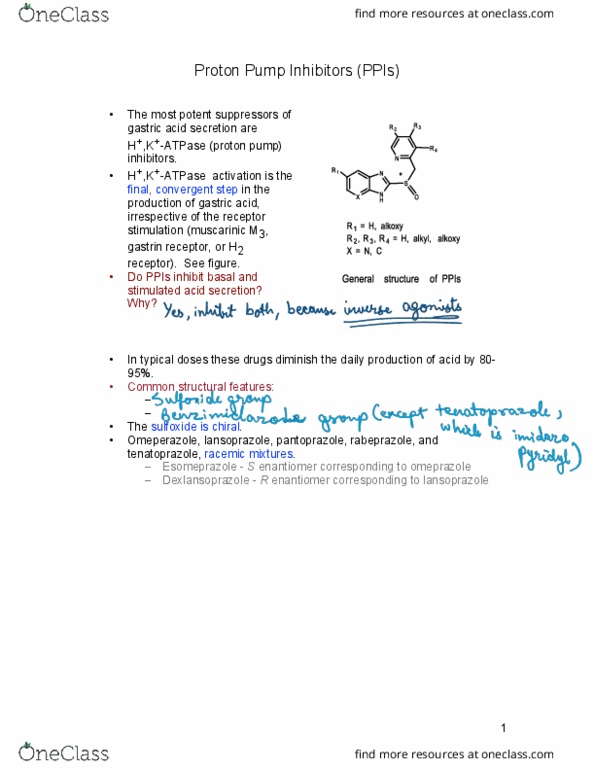
Irreversibly inhibits the h+/ k+ atpase on parietal cells. It is a weak base, and so it works by accumulating in the acidic environment of parietal cell canaliculi. There, it is converted into an achiral form, and so is able to react with, and inactivate, the atpase: following absorption in the small intestine, the drug reaches the parietal cell via the bloodstream. H2 receptor antagonists: ppis consist of a racemic mixture of r and s enantiomers. Omeprazole has both enantiomers, whereas esomeprazole has only one, which makes it have better bioavailoability than omeprazole: esomeprazole and omeprazole have equal benefits for ulcers, but esomeprazole is better than omeprazole for treating gord. Indications: peptic ulcer, reflux oesophagitis, zollinger-ellison syndrome, a component of h. pylori infection treatment. Drug interactions: some inhibition of cp450 ezymes occurs. Cimetidine, famotidine, nizatidine, ranatidine: competitively inhibit histamine and gastrin-stimulated gastric acid secretion by antagonising h2 receptors on parietal cells, reach parietal cells via the bloodstream.