NRS 312 Study Guide - Final Guide: Hypovolemia, Cardiomyopathy, Pallor


Cardiac and Peripheral Vascular
• Cardiac Output and perfusion
o Ability of the heart to pump adequate CO relies on..
▪ Volume of blood in the body
• Problems: hypovolemia
o Dehydration
o Pallor
o Blood loss
▪ Check for pallor, cap refill, level of consciousness, pulses (pedal/radial),
temperature, blood pressure
o Strength and size of the heart muscle
o Electrical conduction leading to valves working and functioning
▪ Hormonal regulation of the heart muscle
o Diameter of the vessels
▪ Atherosclerosis
• Build of and hardening of plaque
o Viscosity of blood
▪ HCT:
• Male:39-50%
• Female: 35-47%
• RBC % to plasma or whole blood
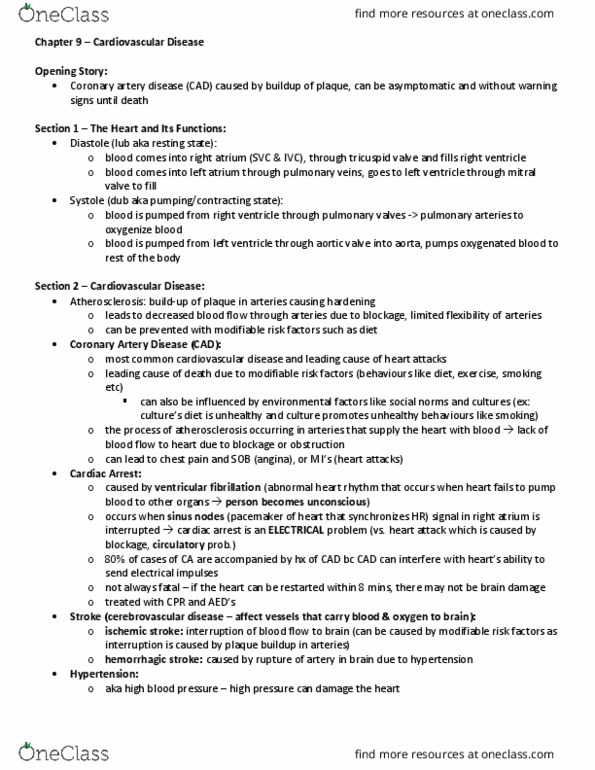
o Cardiac Output: The amount of blood pumped by the heart in one minute
▪ HR x SV=CO
• Subjective Data for Cardiac Assessment
o Ask about Hx: Family Hx of Heart Disease
o Past heart surgeries
o Ask about normal BP
o What medications they are on.
o Hx of hypertension
o Chest pain
▪ Describe the pain
▪ Onest
▪ Scale
▪ Duration
▪ What makes it worse and better
▪ Constant/intermittent
▪ Location and radiation
▪ Experience this exact pain before
o Ask about activity & tolerance.
o Mental, spiritual, emotional -> anxiety/depression
o Diet: Na+, sugar, Processed food
o Hx of alcohol and smoking
▪ Nicotine: vasoconstrictor
find more resources at oneclass.com
find more resources at oneclass.com

• Objective data for a Cardiac Assessment
o Measure B/P
o Heart Rate:
▪ Apical
• Heart sounds and more accurate reading.
▪ Radial or pedal pulse
• Perfusion, strength
o Assess the valves:
▪ Aortic, Pulmonic, tricuspid, and mitral(Appical pulse)-Point of maximal impulse.
• Auscultation
• Cardiomyopathy: left ventricular enlargement
• Point of Maximal Impulse
o (apical pulse) – at the apex of the heart, where you can feel the heart pulsating.
• Extra Heart Sounds
o S3 and S4 = extra heart sounds.
▪ S3 = Occurs immediately after S2, associated with rapid filling of ventricles and
high volume in the atrium: associated with CHF (such as with left ventricular
hypertrophy), pulmonary edema, acute myocardial infarction.
▪ S4 = Occurs just before S1, associated with stiff ventricles that are not flexible
enough to accept blood from atrium; associated with ventricular hypertrophy,
longstanding hypertension with coronary artery disease. Sounds like: a –STIFF’-
wall
• Murmurs, Bruits, and Thrills
o Listen
▪ Murmurs: heard when blood volume is increased in the heart. You are hearing
the large blood volume reverberate or bounce off of the walls of the atrium or
ventricles.
• sounds like whooshing
▪ Bruit: heard over an artery in the neck reflecting turbulence of flow caused by
abnormal narrowing of an artery.
• also over abdominal area. Use bell. Higher pitch sound. partially
occulted blood vessel
o Feel
▪ Thrills: This is something you feel versus hear. Present with murmurs or
abnormalities in the heart itself. Palpate over the apex of heart.
• you can feel over apex of the heart
• Arterial insufficiency
o Look at oxygenated blood meeting the periphery.
o Lack of oxygenated blood
o Pallor or cyanosis
o Cold
o Delayed cap refill
o Intermittent claudication
▪ Cramping pain in lower extremities due to poor circulation of the arterial blood
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Sounds like: a stiff"- wall: murmurs, bruits, and thrills, listen, murmurs: heard when blood volume is increased in the heart. Higher pitch sound. partially: feel occulted blood vessel, thrills: this is something you feel versus hear. Present with murmurs or abnormalities in the heart itself. Palpate over the apex of heart: you can feel over apex of the heart, arterial insufficiency, look at oxygenated blood meeting the periphery, lack of oxygenated blood, pallor or cyanosis, cold, delayed cap refill. Insufficient arterial blood flow in one extremity will cause coolness below the insufficiency. Jugular vein distention: place client flat or at about a 30 degree angle. Observe for jvd visibly distended is normal at a 30 degree angle: sit client up to about a 45 degree angle, observe for jvd visibly distended is not expected and should be referred. Could indicate excess preload and/or right ventricular failure.