PHTY206 Lecture Notes - Lecture 22: Epiphyseal Plate, Ligament, Periosteum


Fractures of the femoral shaft
• MOI
o A high energy or high impact force is usually required to fracture the femur and
therefore this fracture type is most common in young adults
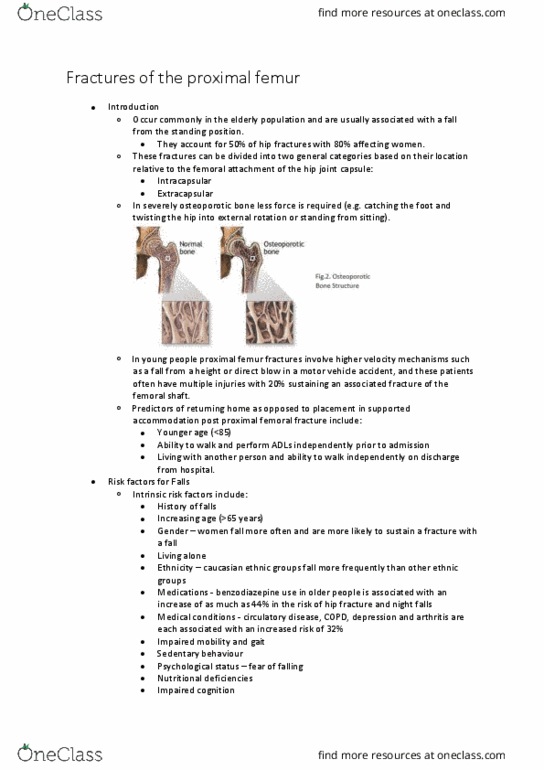
o Low impact fractures of the femoral diaphysis should be considered pathological
until proven otherwise.
o The pattern of the fracture reflects the type of force that caused the injury
• Spiral fracture – rotational force (e.g. foot planted after fall from height upper
body twists the fem
• Transverse and oblique fractures – direct impact or angulation
• Comminuted or segmental fractures – can occur with severe force (often a
combination of direct and indirect forces)
• Associated injuries
o Due to the high energy mechanism of these fractures, there is often significant soft
tissue damage
• Local swelling and haematoma formation between the muscle fascia and soft
tissues may result from the direct injury.
o Displaced fractures can cause nerve damage (femoral nerve), vascular damage or
damage to surrounding muscles.
o Due to the high velocity trauma (MBA/MVA) required to fracture the femoral shaft
the patient has often suffered other injuries from the same accident (e.g. head,
chest, abdomen and pelvis).
o With multiple injuries there is a significant risk of systemic complications including
fat embolism, adult respiratory distress syndrome (ARDS) or multi-organ failure
• Clinical Signs
o Swelling and deformity of the limb is common, particularly with transverse fractures
or compound fractures.
o Movement of the limb is severely limited due to acute pain and muscle spasm.
o Fracture displacement follows a predictable pattern due to the surrounding muscle
• Proximal shaft – proximal fragment flexed, abducted and externally rotated
due to glut med and iliopsoas
find more resources at oneclass.com
find more resources at oneclass.com

• Mid-shaft – proximal fragment flexed and externally rotated but abduction is
less marked
• Lower third – proximal fragment abducted and distal fragment is tilted by pull
of gastrocnemius
o XRAYS
• It is important that the hip and knee are also imaged to identify coexisting
injuries .
• Conservative vs Surgical Management
o Traditionally, traction was the standard treatment for femoral shaft fractures.
• Advantages: simplicity and low infection rates.
• Disadvantage: predominately the length of bed rest required to ensure
adequate healing (10-14 weeks for adults) and the subsequent complications
such as joint stiffness, muscle weakness, circulo-respiratory complications,
and pressure areas
▪ Can also be an expensive treatment option due to the bed cost of
hospitalisation over several weeks.
o Traction may be indicated for:
• Fractures in children
• Patients who cannot tolerate anesthesia
• Departments that lack suitable skill or facilities for internal fixation
• An interim measure whilst awaiting surgical management
o Today surgical management is the treatment of choice for most adults with a
fractured midshaft femur.
• Followed by early mobilisation has several advantages both for the patient
and the health service.
find more resources at oneclass.com
find more resources at oneclass.com

• Early mobilisation significantly lowers the risks associated with prolonged bed
rest, whilst allowing the patient to regain joint ROM, muscle strength and a
normal gait pattern.
• If patients have suffered multiple injuries including severe chest trauma,
surgery to introduce a reamed intramedullary nail may have an adverse effect
when performed within the first 24 hours of fracture
▪ For these patients it may be appropriate to stabilise early with an
external fixator and proceed to insertion of an intramedullary nail at a
later stage he the patiet’s oditio has stailised
• Conservative Management Traction
o Usually involves immobilisation of the leg in a traction device
o A traction force is usually applied through a skeletal pin (often a Steinman or
Denman pin) however skin traction may be applied for short periods.
o The traction force should maintain adequate reduction of the bone ends whilst not
retarding the healing process.
o Physiotherapy Management during Traction
• Daily circulo-respiratory assessment and maintenance exercises
• Monitoring and advice on management of potential pressure areas
• Exercises to strengthen the upper limbs (this may involve the use of free
weights or resistance band)
• Exercises to maintain strength in the unaffected leg
• Active and passive exercises for the ankle of the affected limb to avoid
gastroc/soleus shortening and a loss of dorsiflexion range of motion
• At 4-6 weeks post-operatively, callous formation at the fracture site
(confirmed by the surgeon on x-ray) may allow the commencement of hip and
knee range of motion and gentle strengthening exercises.
• If the patient remains in traction it may be possible to use the split bed
technique, as seen in the picturebelow, to remove a portion of the bed and
allow for knee flexion and quadriceps strengthening exercises.
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Lower third proximal fragment abducted and distal fragment is tilted by pull of gastrocnemius: xrays. If patients have suffered multiple injuries including severe chest trauma, surgery to introduce a reamed intramedullary nail may have an adverse effect when performed within the first 24 hours of fracture. If the patient remains in traction it may be possible to use the split bed technique, as seen in the picturebelow, to remove a portion of the bed and allow for knee flexion and quadriceps strengthening exercises. Interlocking screws are used to increase stability: physiotherapy management. Initial post-operative physiotherapy management will include: daily circulo-respiratory assessment and maintenance exercises. Surgical management - orif- plate fixation: plate fixation may be indicated for: Fractures with periarticular or intra-articular damage which precludes the insertion of an intramedullary nail. Fractures in a growing child (able to be applied without disrupting the growth plates).