MEDS12003 Lecture 2: SS week 2 notes


1 | P a g e
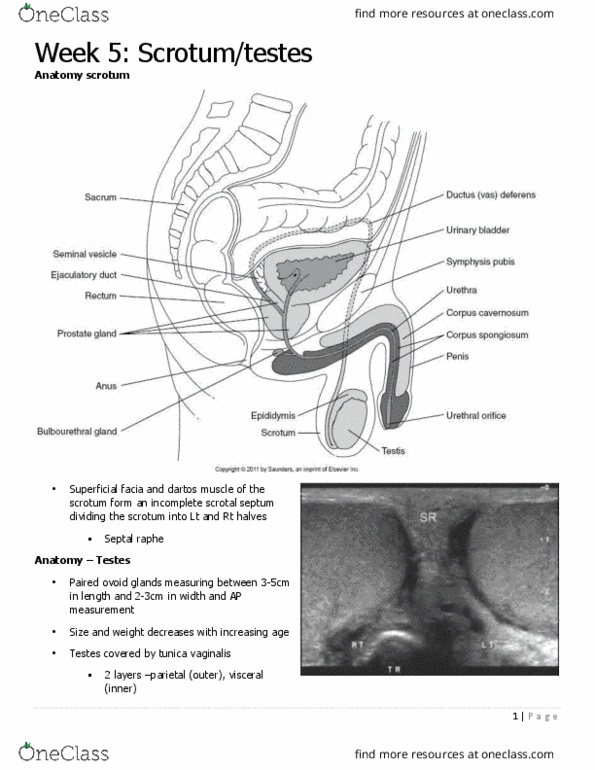
Week 2: Thyroid gland
Normal thyroid – Lt lobe
• paired right and let lobes
• Isthmus – midline
• Pyramidal lobe – 10-40%
• Each lobe <2cm in AP and TSV
• Isthmus 4-6cm
• Paired right and left lobes joined midline at
the isthmus.
• Pyramidal lobe only seen in some patients
and atrophies with age
find more resources at oneclass.com
find more resources at oneclass.com

2 | P a g e
Sonographic features
• Size
o Lat lobe … 4 - 6 cm. L, 3 – 6 cm. W, 1.4
– 1.8 cm. AP
o Isthmus … 4 - 6 mm. AP
• Shape
o ovoid
• Echogenicity
o very homogenous, hyperechoic to
surrounding structures
• Contour
o smooth (capsule)
Thyroid gland arises from thyroid sac –diverticulum
which thickens in 3rd week of embryonic
development. Stalk between thyroid and tongue is
thyroglossal duct which opens in the embryo at the
Foramen cecum. Thyrogloassal duct atrophies by 6th
week, follicles form 8th week. Thyroglossal duct
normally closes after birth. Ectopic thyroid tissue
can be found anywhere along the descent from
Foramen cecum to the 1st tracheal ring.
Normal variants
• Agenesis
• Incomplete descent
• Pyramidal lobe –accessory lobe
• Incomplete isthmus
• Thyroglossal duct cyst
Physiology
• Endocrine gland -secretes hormones
o T3
o T4 –thyroxine
o Calcitonin
• Secretion controlled by TSH –pituitary gland
• Controls the basal metabolic rate (BMR)
o the amount of energy the body expends maintaining life
• Necessary for growth & development
T3 –Triiodothyronine, Thyroxine is the primary hormone of the thyroid. When thyroid hormone is needed,
TSH is secreted by the anterior pituitary gland which releases hormones into the bloodstream. Control of
TSH is regulated by thyrotropin-releasing factor produced in the hypothalamus. Decrease in BMR>low
thyroid hormone concentration>Increase in TRF causes inc in TSH and inc in thyroid hormones>restores
balance.
Figure 1Embryology
find more resources at oneclass.com
find more resources at oneclass.com

3 | P a g e
Laboratory values
Thyroid scan
• What is expected from the thyroid scan?
o Screening
▪ Location of lesions, cystic vs solid
o Differentiate between:
▪ Generalised disease
▪ Multi-nodular disease
▪ Solitary lesions
o FNA guidance
Clinical indicators
• Abnormal thyroid hormone results (TSH, T4, T3)
• MNG (Multinodular Goitre)
• Lump in throat on swallowing
• Tightness in throat
• Follow up from previous imaging
Pathology
• Nodular Thyroid Disease
▪ Hyperplasia and Multi-Nodular Goitre
▪ Malignant thyroid disease
o Most common thyroid disease
o Thyroid cancer is rare → Thyroid Ca < 1% of all malignant neoplasms
o Most nodules are benign
• Diffuse Thyroid Disease
o Hashimoto’s Thyroiditis
o Graves’ Disease
70% of focal thyroid nodules are SOLID 4-7% of the adult population in the U.S. have palpable thyroid
nodules. Increased risk with exposure to ionizing radiation
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Isthmus midline: paired right and let lobes, pyramidal lobe 10-40, each lobe <2cm in ap and tsv, paired right and left lobes joined midline at. Isthmus 4-6cm the isthmus: pyramidal lobe only seen in some patients and atrophies with age. Sonographic features: size, lat lobe 4 - 6 cm. Ap: shape, ovoid, echogenicity, very homogenous, hyperechoic to surrounding structures, contour, smooth (capsule) Thyroid gland arises from thyroid sac diverticulum which thickens in 3rd week of embryonic development. Stalk between thyroid and tongue is thyroglossal duct which opens in the embryo at the. Thyrogloassal duct atrophies by 6th week, follicles form 8th week. Ectopic thyroid tissue can be found anywhere along the descent from. Incomplete descent: agenesis, pyramidal lobe accessory lobe, thyroglossal duct cyst. Physiology: endocrine gland -secretes hormones, t3, t4 thyroxine, calcitonin, secretion controlled by tsh pituitary gland, controls the basal metabolic rate (bmr) the amount of energy the body expends maintaining life, necessary for growth & development.