CSB520 Lecture Notes - Lecture 12: Glycogen, Sympathetic Nervous System, Exophthalmos


Week 12 - Endocrine & Skin Pathology
Tuesday, 7 June 2016 4:41 PM
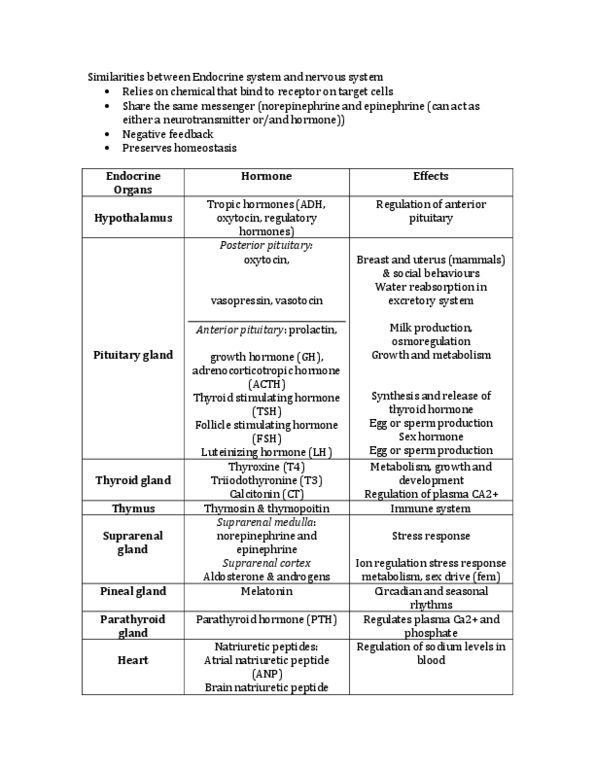
Endocrine GlandsEndocrine Glands
•Classical - ductless exocytose into extracellular space --> plasma
○Pituitary
○Thyroid
○Parathyroid
○Pancreatic islets
○Adrenal glands
○Ovaries
○Testes
•Non-traditional
○Heart (natriuretic peptides)
○Kidney (renin, EPO)
○Gut (incretins, cholecystokinin or CCK)
○Adipose (leptin, adiponectin, visfatin, etc. etc.)
Hormone StructureHormone Structure
•Proteins (ACTH)
•Peptides (vasopressin)
•Monoamines (noradrenalin)
•Amino acid derivatives (triiodothyronine)
•Steroids (cortisol)
•Lipids (prostaglandins)
ActivitiesActivities
•Protein, peptide, monamine
•Lipophilic
•Act on protein receptors at the cell surface
○Receptors will trigger events inside the cell
○Can have very long term effects
•Steroid & thyroid
○Includes vitamin D - cross talk at the level of the nucleus
•Nuclear receptors
Regulation of Plasma LevelsRegulation of Plasma Levels
•Regulation of hormone levels
•Hormone biosynthesis - how much is being made
•Precursor processing - some hormones require processing
•Hormone release - stimulus triggering release
•Hormone-binding in plasma
•Hormone metabolism

Negative FeedbackNegative Feedback
•How a lot of hormones are regulated
•Hypothalamus --> TRH --> Anterior pituitary
•--> TSH -- > acts on the thyroid (in this case)
•--> T3 and T4
•--> Target tissues
•Negative feedback! Turn off stimulus
How does endocrine disease develop?How does endocrine disease develop?
•Hormone deficiency
○Primary due to decrease in production by a gland
○Secondary due to decrease in trophic hormone production
•Hormones that have other endocrine glands as their target
•Hormone excess
○Primary due to increased production by a gland
○Secondary due to increased trophic hormone production
•Tumours
○Local pressure & invasion
○Non-functional lesion
○Functional lesion
•Resistance to hormone effects
○Target organ resistance
•E.g. type 1 diabetes
○Failure to activate hormone
Pituitary GlandPituitary Gland
•Located at the base of the brain
•Role in nervous & endocrine system
•Secretion of all hormones is controlled by hypothalamus & feedback
loops
•Anterior + posterior originate from 2 different sources during
embryogenesis
○Evident by different structure & functions
Hormones of the Pituitary GlandHormones of the Pituitary Gland

Prolactinomas & ProlactinaemiaProlactinomas & Prolactinaemia
•Most common tumour affecting pituitary
○Predominantly weakly acidophilic & chromophobic cells
○Leads to increase of prolactin levels = prolactinaemia
•Amenorhea, galactorrhea, loss of libid & infertility
Growth Hormone AdenomasGrowth Hormone Adenomas
•Second most common form of pituitary adenoma
•Persistent increase of GH secretion -> insulin-like growth factor 1 -->
causes clincial manifestations
○If adenoma presents in childhood before epiphyses close -->
gigantismgigantism
○If adenoma presents in childhood after closure of epiphyses -->
acromegalyacromegaly
•
Prolonged
elevated GH also leads to:
○Diabetes
○Gonadal dysfunction
○Arthritis
○Hypertension
○CHF
○Generalised muscle weakness
○Increased risk of GIT cancers
Other Pituitary AdenomasOther Pituitary Adenomas
•Corticotroph cell adenoma --> ACTH
○Hypercortisolism --> Cushing syndrome
•Gonadotroph adenomas --> LH & FSH
•Thryotrophic adenoma --> TSH
•Non-functioning adenomas:
○Clincially silent versions of functioning adenomas discussed
○Pituitary carcinomas:
•Rare & mostly non-functional
•Can be poorly or well differentiated
•Usually diagnosed when metastases are detected elsewhere
Thyroid GlandThyroid Gland
•Has 2 lobes, located below & anterior to pharynx
○Hypo/hyperthyroidism, goitre, neoplasms (adenoma & carcinoma)
and congenital disease
Document Summary
Endocrine glands: classical - ductless exocytose into extracellular space --> plasma. Hormone structure: proteins (acth, peptides (vasopressin, monoamines (noradrenalin, amino acid derivatives (triiodothyronine, steroids (cortisol) Lipophilic: act on protein receptors at the cell surface. Receptors will trigger events inside the cell. Can have very long term effects: steroid & thyroid. Includes vitamin d - cross talk at the level of the nucleus: nuclear receptors. Regulation of plasma levels: regulation of hormone levels, hormone biosynthesis - how much is being made, precursor processing - some hormones require processing, hormone release - stimulus triggering release, hormone-binding in plasma, hormone metabolism. Negative feedback: how a lot of hormones are regulated, hypothalamus --> trh --> anterior pituitary. -> tsh -- > acts on the thyroid (in this case) How does endocrine disease develop: hormone deficiency. Primary due to decrease in production by a gland. Secondary due to decrease in trophic hormone production: hormones that have other endocrine glands as their target, hormone excess.