PHRM4012 Lecture Notes - Lecture 3: Cytochrome P450, Simvastatin, Fluvastatin

25 Jul 2018
School
Department
Course
Professor
Document Summary
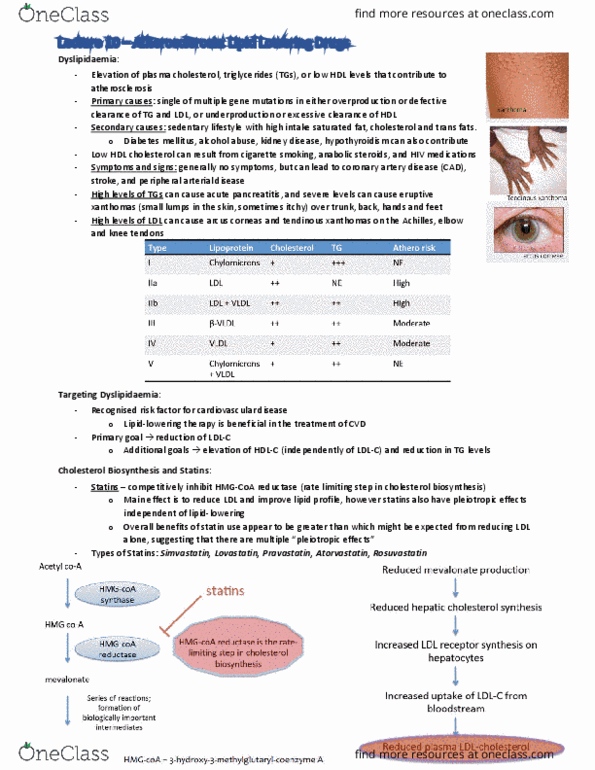
Dyslipidaemia risk of cardiovascular disease increases with raised lipid levels. Secondary causes of dyslipidaemia: alcoholism, diabetes mellitus, hypothyroidism, obesity, renal insufficiency, drugs, beta-adrenergic blockers, bile acid-binding resins, eostrogens ticlopidine levels change in 2-3 weeks, stabilize in 1-3 months. Secondary dyslipidaemia: diabetes/obesity/smoking/renal impairment increased tg, decreased hdl, hypothyroidism/anorexia/cholestasis increased ldl, alcohol/eostrogen increased tg. Combos: statins + ezetimibe fibrates + ezetimibe. Statins inhibits hmg-coa inhibits cholesterol production/increases hepatic uptake decreased ldl, tg, slight hdl increase. Doubling dose = 5-10% reduction in ldl. Hepatobiliary/muscle problems frail, elderly >80 years old. Myopathy increases with asian, female, cyp450 inhibitors. Atorvastatin label 18 10-80mg (2nd most potent) Simvastatin label 18 10-80mg (most side effects with same efficacy with others) First line if statins not tolerated/add if ldl uncontrolled. Se constipation, gi upsets, changed liver function tests, increased tg. Addition to statin= 5-10% ldl reduction first line for high tg. Se increased risk of rhabdo with statins, photosensitivity, gi. Best taken half an hour before food.