PHIL 235 Lecture Notes - Lecture 3: Anarchism In Russia, Relativism, Mexican Americans

11 May 2018
School
Department
Course
Professor

Lesson 3.1 –Notes
Different Standards of Competence
A minimal standard of competence
• The patient merely is able to express a preference.
• Not in fact a criterion of competent choice at all
• Its ignores if mistakes or defects are present when the reasoning process
leading to the choice → good or bad for them or maybe even harmful
• Fails to protect patients well-being
An outcome of Standard of Competence
• Standards that only look at the outcome or content of the decision
• Example: the standard that the choice be a reasonable one, or be what other
reasonable or rational persons would choose.
• Failure of patients choice
• Protects the patients well-being only to point where the standard conception
of well-being
• Fails to respect self-determination
• Any standard of individual well being that does not ultimately rest on an
individual’s own underlying and enduring aims and values is both
problematic in theory and subject to in- tolerable abuse in practice.
A process Standard of Decision-Making Competence
• An adequate standard of competence will focus primarily not on the content
of the patient’s decision but on the process of the reasoning that leads up to
that decision
• 2 central questions for any process standard of competence:
1) A process standard must set a level of reasoning required for the patient to
be competent → how well must the patient understand & reason to be
competent? Understanding can be limited or reasoning can be defective,
and can this be considered competent?
2) How certain must those persons evaluating competence is about how well
the patient has understood and reasoned in coming to a decision?
Relation of the Process Standard of Competence to Expected Harms and Benefits
• There is no standard competence because it varies case to case
find more resources at oneclass.com
find more resources at oneclass.com

• This is true because
(1) The degree of expected harm from choices made at a given level of
understanding and reasoning can vary from none to the most serious,
including major disability or death, and because
(2) The importance or value to the patient of self-determination can vary
depending on the choice being made.
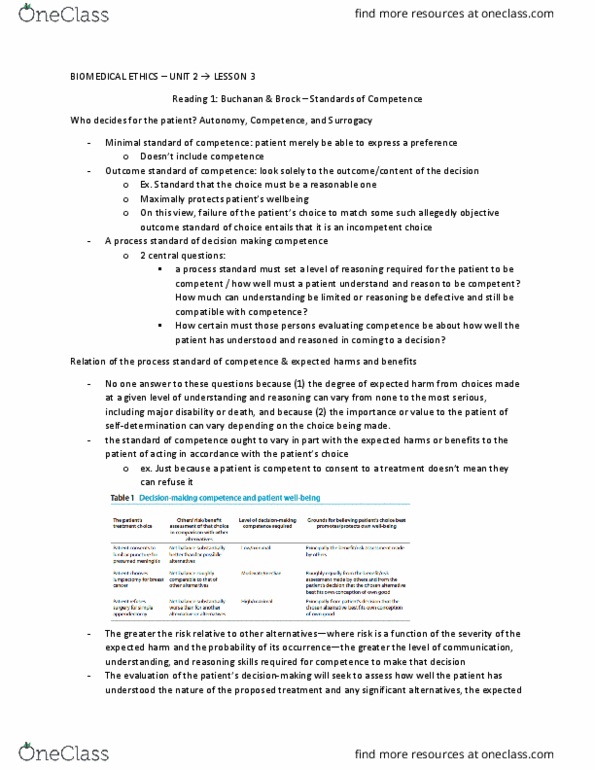
• Standard of competence ought to vary in part with the expected harms or
benefits to the patient of acting in accordance with the patient’s choice
Example: just because a patient is competent to consent to a treatment, it
does not follow that the patient is competent to refuse it, and vice versa.
Example: consent to a low-risk lifesaving procedure by an otherwise
healthy individual should require only a minimal level of competence, but
refusal of that same procedure by such an individual should require the
highest level of competence.
• Because the appropriate level of competence properly required for a
particular decision must be adjusted to the consequences of acting on that
decision, no single standard of decision-making competence is ad- equate
• Thus, according to the concept of competence endorsed here, a particular
individual’s decision-making capacity at a given time may be sufficient for
making a decision to refuse a diagnostic procedure when forgoing the
procedure does not carry a significant risk, although it would not
necessarily be sufficient for refusing a surgical procedure that would
correct a life-threatening condition. The greater the risk relative to other
alternatives where risk is a function of the severity of the expected harm
and the probability of its occurrence—the greater the level of
communication, understanding, and reasoning skills required for
competence to make that decision.
• Crude but perhaps helpful way of characterizing the proper aim of the
evaluator of the competence of a seemingly harmful or “bad” patient choice
is to think of him or her addressing the patient in this fashion: “help me try
to understand and make sense of your choice. Help me to see whether your
choice is reasonable, not in the sense that it is what I or most people would
choose, but that it is reasonable for you in light of your underlying and
enduring aims and values.” This is the proper focus of a process standard of
competence.
find more resources at oneclass.com
find more resources at oneclass.com

Lesson Notes 3.2
Involving Children in Medical decisions
• Just as the concept of informed consent has developed over the last 30
years with respect to competent adult patients, so new ways of thinking
about the role of children in medical decision-making have evolved.
• A family-centered approach→ yes child’s developing autonomy is
important but a FCA is the best model for understanding the interdependent
relationships that bear upon the child’s situation
• Family centered approach → challenge when parents and child disagree.
• Integrity in this relationship is fundamental to the achievement of the goal
of medicine, which has been defined as “right and good healing action
taken in the interest of a particular patient.”
• The care of children, on the other hand, has been described in terms of a
“triadic” relationship in which the child, his or her parents, and the
physician all have a necessary involvement
• → When there is disagreement between parent and child, the physician may
experience some moral discomfort in having to deal separately with the
child and parent
• Usually the assumption that parents know best is sound but its not always
the case, and simply respecting the parents wishes in these cases is
inadequate.
• This approach does not discount the parents’ concerns and wishes, but
recognizes the child as the particular patient to whom the physician has a
primary duty of care. This approach seeks to harmonize the values of
everyone involved in making the decision.
The law
• The legal right to refuse medical treatment is related to, but not identical
with, the right to consent to treatment.
• Patient is allowed to refuse even life-saving medical treatment in Canadian law.
• In common law the notion of the “mature minor” rec- ognizes that some
children are capable of making their own health care choices despite their
age.
• In the case of children who are incapable of making their own health care
decisions, parents or legal guardians generally have the legal authority to
act as surrogate decision-makers.
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
A minimal standard of competence: the patient merely is able to express a preference, not in fact a criterion of competent choice at all. Its ignores if mistakes or defects are present when the reasoning process leading to the choice good or bad for them or maybe even harmful: fails to protect patients well-being. Example: just because a patient is competent to consent to a treatment, it does not follow that the patient is competent to refuse it, and vice versa. This approach seeks to harmonize the values of everyone involved in making the decision. The law: the legal right to refuse medical treatment is related to, but not identical with, the right to consent to treatment, patient is allowed to refuse even life-saving medical treatment in canadian law. In common law the notion of the mature minor rec- ognizes that some children are capable of making their own health care choices despite their age.