NSG 2317 Lecture Notes - Lecture 6: Paroxysmal Nocturnal Dyspnoea, Mitral Valve, Presyncope

10 Oct 2018
School
Department
Course
Professor
Health Assessment 2317
Notes: Lecture 6
Prof: P. O’Byrne
Circulatory system
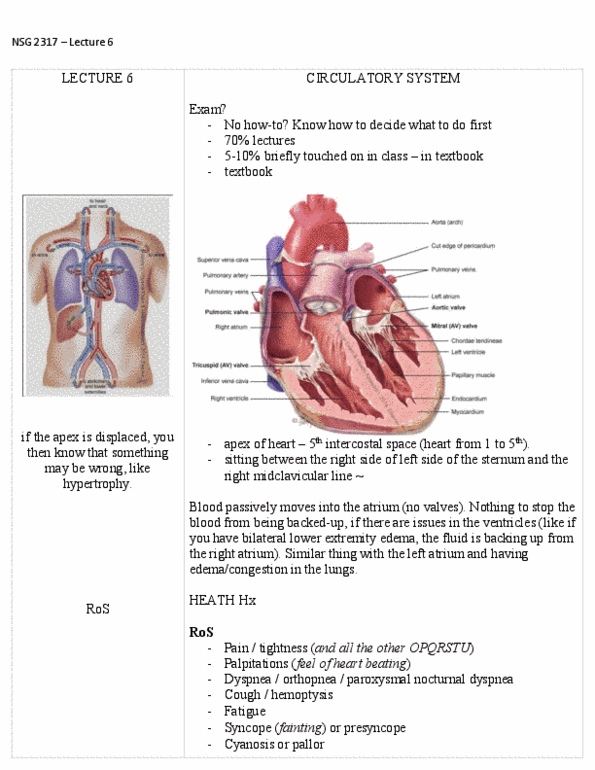
• Position and landmarks
o Mediastinum
o Precordium: space between the heart and the actual rib cage
o Apical impulse: place at the apex where you can feel as pulse, you can detect if
there is disease depending on the location and …
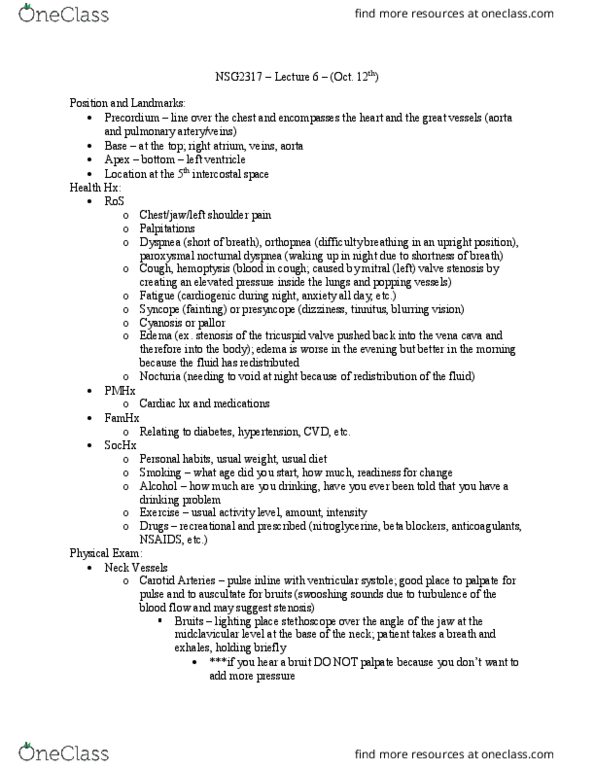
• Anatomy review
o Atria: holding room for the ventricles, atrial kick is blood expelling into the
ventricle (lub), closing of the valves is the (dub)
o Mitral valve between left and right ventrica
o No valve between the inferior vena cava and superior vena cave and the right
atrium
Health history
• ROS
o Pain, tightness, palpations, dyspnea, orthopnea, paroxysmal nocturnal dyspnea,
cough, hemoptysis (things backing up and overwhelm the capillaries), fatigue,
syncope or presyncope, cyanosis or pallor, edema/weight gain (fast fluid
retention,) nocturia (peeing a lot at night)
o Chest pain is the top syndrome of for MI, the rest women exceed
o Atypical symptoms are more common in women which is bad because they
usually get overlooked for something else
• PMHx
o Cardiac history, medications
• FamHX
o Cardiac history
• SocialHx
o Personal habits
Physical exam
• Neck vessels
o Right external and internal jugular
o Arteries usually used to palpate the pulse, if feel something else there (feels
unusual or the person notes a certain symptom like ringing in their ears,
presyncope or syncopy) then you auscultate in order to listen for whistling or
other sounds
• Carotid arteries
• Jugular venus pressure
o Checking for heart failure
o No two people will come up with the same thing
o Put the person between 30-40 degrees and turn their head to the left because
you want the right jugular
o Right side can’t handle fluid return from systemic circulation and will back up
into the neck, you want to know how high the fluid goes
o Push into the liver which will dump blood into the circulatory system
• Precordium
o Checking for heaves and trills***
o You should feel the heart moving and no other sensations
• Apical pulse
o 1. Normal healthy heart
o 2. Left ventricle thickens, caused by hypertension, major problem there is that
the lumen/space is a lot smaller, the blood that can go into the left ventricle and
that can be expelled is a lot smaller meaning that the heart has to pick up its
pace in order to compensate. Everything else changes as well with the
thickening, the valves might not touch perfectly anymore and might have blood
flowing back
o 3. Heart dilates, might be the outcome of a heart attack, there is structural
damage to the heart which causes it to expand. It can take in a lot of blood but
the issue is that it can’t contract with force
• Percussion
o Not normal done • Not accurate
o More accurate methods available
• Auscultation
o Left lateral position is the best because it pushesthe heart to rib cage so now
everything is louder
• Auscultation areas
o Where you listen to the sound is not exactly where the valve is
o Sound will follow the blood flow, you’re listening for the sound as it moves
through
o Right sternal border = aortic area, blood comes up from the left ventricle so that
is where you will hear it
o Left sternal border= pulmonic area, blood mores up
o 4th intercostal space = tricuspid, blood shifts
o Apical pulse = mitral area, blood moves down
o Move stethescope along Z-pattern
• Auscultation components
o Rate & rhythm (regular, irregular/regular-irregular or irregular irregular)
strength, bradycardia, tachycardia)
o S1S2: closure of mitral valves and closure of pulmonic valves **** (the lubdum)
o S3S4: extra sounds, things added to the lubdub
o Murmurs
Document Summary
Everything else changes as well with the thickening, the valves might not touch perfectly anymore and might have blood flowing back: 3. Heart dilates, might be the outcome of a heart attack, there is structural damage to the heart which causes it to expand. Irregular: sinus arrhythmia are normal, heart can speed up with increase respiratory pattern, linked to inspiration, sequestering blood, blood return to the heart. I(cid:374) (cid:271)et(cid:449)ee(cid:374) these t(cid:449)o is (cid:449)here (cid:455)ou"ll feel the pulse flow. The o2 demand goes up and sends out for more o2 (cid:271)ut it (cid:272)a(cid:374)"t (cid:272)o(cid:373)e i(cid:374) (cid:271)e(cid:272)ause the ste(cid:374)oti(cid:272) (cid:448)al(cid:448)e is so stiff, gets lefts ventricular h(cid:455)pertroph(cid:455). It"s goi(cid:374)g to (cid:271)e a loud (cid:373)ur(cid:373)ur, (cid:373)id-systolic, loudest are right sternal border and radiates into the neck: mitral stenosis: same pro(cid:271)le(cid:373)s are aorti(cid:272), e(cid:454)(cid:272)ept it"s the (cid:448)al(cid:448)es (cid:271)et(cid:449)ee(cid:374) the atrium and ventricles. Not a lot of symptoms, dyspnea on exertion, angina, inadequate o2 supply: mitral regurgitation: same as aortic, symptoms include dyspnea on exertion.