Background
Almost all animal and plant cells require oxygen and give off carbon dioxide. This is called gas exchange and it occurs by passive diffusion. Some animals do all or most of their gas exchange across their skin (for example amphibians) but they have very low metabolisms and use very little oxygen and get rid of very little carbon dioxide.
On the other hand humans (and other mammals) have very high metabolic requirements and we canât rely on gas exchange over the limited 1.5 to 2.0 square meters of our skin to get enough oxygen in and carbon dioxide out fast enough. Our gas exchange takes place across a very thin membrane in the Alveoli of the lung and the gas exchange surface in humans is estimated to be between 50 and 100 square meters, or between 25 and 67 times our skin surface area.
Our lungs provide a huge surface for gas exchange but they are a dead-end system. Once the oxygen in the lungs is used up it needs to be replenished and carbon dioxide builds up in the air spaces in the lungs and needs to get out. This is where the diaphragm and a few of the skeletal muscles become important. In its relaxed state the diaphragm is at its longest and the space in the thoracic cavity (and the lungs) is small. When the diaphragm contracts it shortens, which increases the volume of the thoracic cavity (and the lungs). The increase in size means the pressure is lower in the lungs than outside so air comes into the lungs (inhalation). As the diaphragm relaxes, the lungs decrease in size enough that the pressure inside the lungs is higher than the external air pressure so air comes out (exhalation).
Introduction
In this lab you will be building a model of a lung and experimenting with different ways to breath.
Supplies:
In the Lab Kit
One round 9" balloon (one lung, we donât need two for this)
medium-sized plastic bag large enough to fit over bottom end of bottle (diaphragm)
medium-size, thin rubber band
You supply
plastic 2-liter soda bottle with bottom cut off (thoracic cavity)
Tape (optional)
Directions:
1. Insert the balloon through the open bottom of a modified 2-liter soda bottle and up over the neck of the bottle. Pull the end of the balloon over the edges of the neck of the bottle. The balloon is held open by the neck of the bottle.
2. Place the plastic bag over the bottom (open) end of the 2-liter bottle and use the rubber band to hold it in place. This will serve as the diaphragm. To inflate the lung, blow into the balloon just before you fasten the rubber band. You can also wrap tape over the edges of the plastic bag to minimize air leaks
3. Grasp the bottom of the plastic bag and pull it down and push it up. Watch as the "lungs" (the balloon) expand and contract as you do this. The balloon has to change size because the air space between the balloon and bottle must remain constant. (Well, it would if the seal around the plastic bag and bottle were perfect).
You may block the "trachea" (the neck of the bottle) so that the air supply is cut off and watch as nothing happens when the "diaphragm" is pushed in and out.
This model isnât perfect. None of the joints are air tight as they would be in a real thoracic cavity. Pull the âdiaphragm down and watch the lungs expand . If you hold it in place, the lungs will collapse again over time. This is because of leaks and is not how real lungs work. Pushing the diaphragm in and pulling it out over and over does give you an idea of how lungs work. As the diaphragm tightens, contracts (pull down on the plastic bag) the lungs fill with air. As the diaphragm relaxes (push up on the plastic bag) air is expelled from the lungs .
There are several different ways we breath, i.e. expand our thoracic cavity so that our lungs can expand. You have just made a demonstration model of the diaphragm at work. You can also use your rib cage to expand and contract so that you can inhale and exhale. There are muscles between and around your ribcage which you can use to change the size of your thoracic cavity.
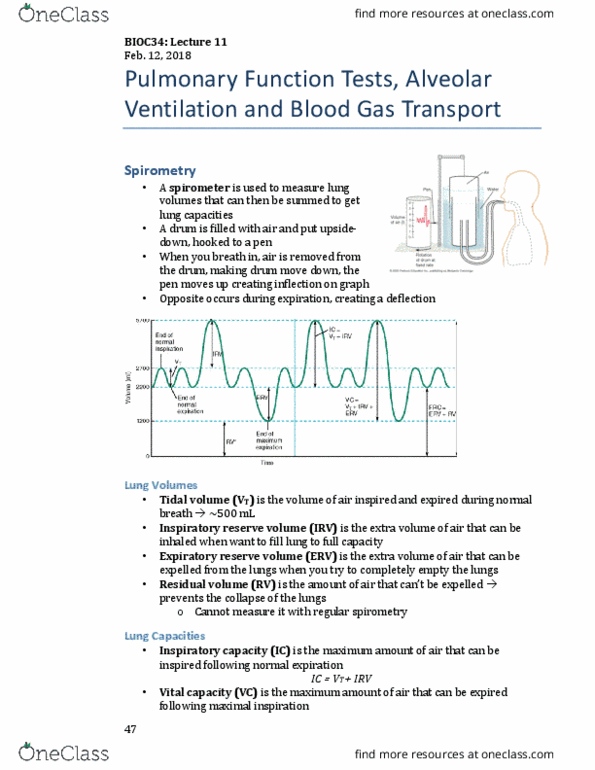
This is approximately what your model of a lung will look like.
Answer the questions on the Report Page
Report Page Name
1. Put a hand on your lower ribcage and try moving your ribs out and in. Does air also move in and out?
2. Someone with an upper back or neck injury may not have the options of using diaphragm or ribs to breath. They can learn to use the clavicle and the muscles attached to expand their thoracic cavity a small amount and breathe independently for short periods of time. Put your hand on you clavicle and try to raise and lower just that bone without using your diaphragm or your ribs. It isnât easy but you should be able to get a little air into and out of your lungs this way. How effective do you think this way of breathing is?
3. When you take a really deep breath you use all these muscle groups to help. Take a really deep breath and notice that your ribs expand, your lower abdomen comes out (a sign that the diaphragm has contracted) and your shoulders lift a little (the upper chest and clavicle are working). Now take a relaxed breath. Only your abdomen should go in and out. The movement of your abdomen is a result of the contracting diaphragm pushing on the contents of your âgutâ which forces your abdomen to push out.
Do you breath in or out when your diaphragm contracts?\
4. If a hole were poked in your thoracic wall (the wall of the pop bottle â the hole should be at least the diameter of a pencil)
a. what would happen when you tried to breath? (This is a pneumothorax).
b. Is the space between the balloon and plastic bottle still required to remain constant?
5. Would it be possible to live with a paralyzed diaphragm? Explain your answer.