PSY493H1 Lecture Notes - Lecture 3: Visual Cortex, Lateral Geniculate Nucleus, Inferior Temporal Gyrus



Retina
Takes raw input of light (membrane polarization)
-
Light -> ganglion cells -> amacrine cell -> bipolar cell ->horizontal cell -> cone/rod
-
Photoreceptors: Rod & Cones
Light energy -> electrochemical energy
-
120 M rods vs. 6 M cones (more rods than cones)
Rods (abundant in retina)
Contain pigment Rhodopsin
§
Sensitive to small amount of light (in the dark)
§
Detect black, white and grey
§
Located in the periphery of the fovea
§
Many rods connect to one ganglion cell
§
○
Cones (sparse in retina)
3 different pigments called photopsins
Short wavelength -> blue □
Medium wavelength -> green□
Long wavelength -> Red □
§
Sensitive to large amount of light
§
Detect Color
§
Located at mostly at fovea
§
Few cones to ganglion (specificity)
§
○
-
Fovea
Huge concentration of cones
○
-
Rods vs. Cones
Rods are more useful at low light levels
Many rods to each ganglion cell = less resolution
§
○
Cones are better for detecting colour and detail
Few cones to each ganglion cell = more resolution
§
○
-
Receptive field
Area of space where a neuron maximally fires
-
Neuron is said to prefer a given stimulus
-
Also true for auditory, somatosensory systems
-
Center-surround Receptive Fields
Each cell has an excitatory and inhibitory area of sensitivity
-
On-center = activated
-
Off-center = deactivated
-
Ganglion cells (innervate the Lateral Geniculate Nucleus (LGN))
Some processing at the retina!
-
M cells (Parasol) -> magnocellular layer of LGN
Motion, B&W(rods), fast, large receptive fields!
○
-
P cells (Midget) -> parvocellular layer of LGN
Precise, colour (cones), slow, small receptive fields!
○
-
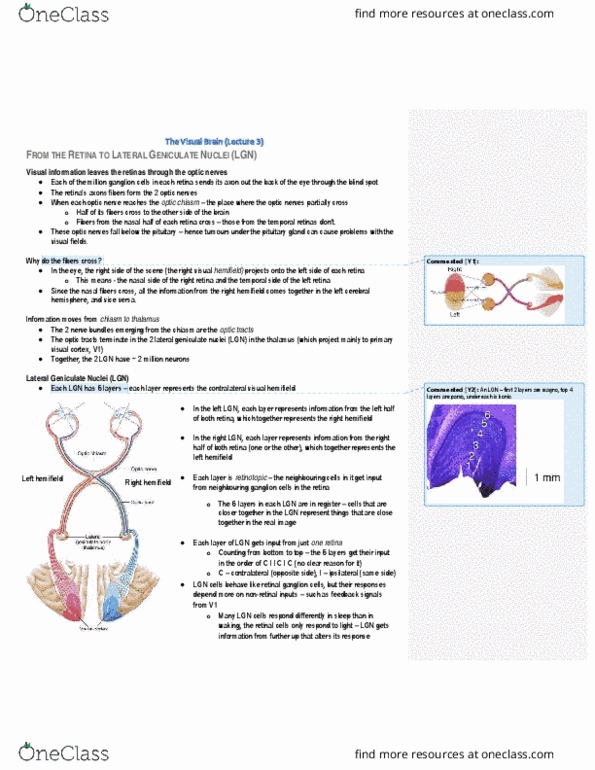
Visual pathways
Contralateral organization of visual pathways
-
Info from the right visual field is directed solely to the primary visual cortex (V1) on
the left hemisphere (left visual field to right hemisphere)
-
From Retina to Brain
Two main pathways
Tectopulvinar path
○
Geniculostriate path (LGN)
○
-
Tectopulvinar pathway
Retina -> superior colliculus -> pulvinar -> extrastriate cortex (V2)
Sensitive to motion and novelty
§
Contains 10% of optic nerves
§
Receives input from M cells
§
Sensitive to periphery, not fine detail
§
Automatic eye movement orientation
§
○
-
Geniculostriate pathway (LGN path)
Retina -> lateral geniculate nucleus 0 -> primary visual cortex (V1, striate
cortex)
Sensitive to colour and fine grained detail
§
Contains 90% of optic nerves
§
Receives input from M & P cells
§
○
-
LGN visual pathway
How does the brain convert sensory signals into the coherent objects we perceive?
Right nasal and right temporal -> left LGN
○
Left nasal and left temporal -> right LGN
○
-
Ipsilateral eye projects to layers 2, 3, 5
-
Contralateral eye to projects to layers 1, 4 and 6
-
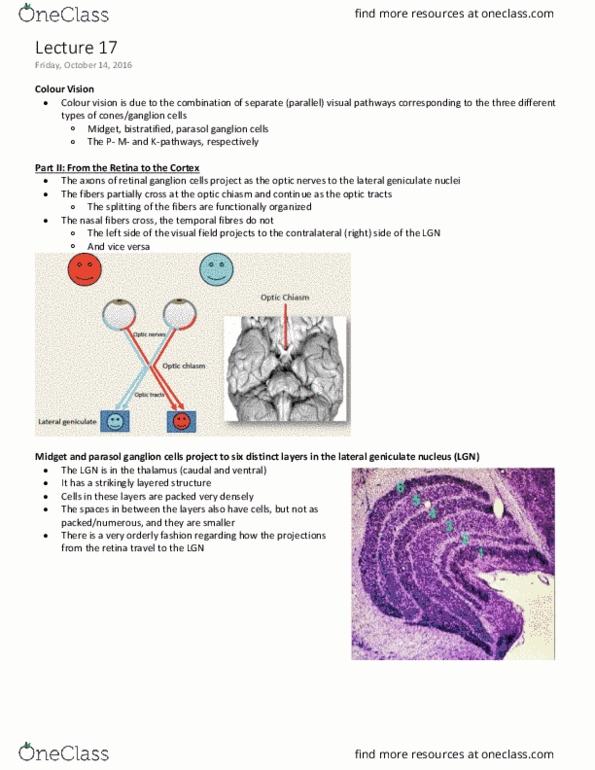
Lateral Geniculate Nucleus (LGN)
Properties of LGN: Morphonogy
Not all retinal maps the same
○
M & P origins are maintained in LGN
Parvocellular layers
Receive input from midget ganglion cells (P cells) in the retina
Cone input predominates
®
□
Small cells
□
Top 4 layers (3, 4, 5, 6)
□
§
Magnocellular layers
Receive input from parasol ganglion cells (M cells) in the retina
□
Large cells
□
Bottom 2 layers (1, 2)
□
§
○
-
Retinotopic Organization
Two paths within LGN
Magnocellular Pathway Parvocellular pathway
M cells
-
Color insensitive
-
Large receptive fields
-
Fast, transient
-
More sensitve at low contrest/ low spatial
frequency
-
ACTION! (parietal lobe)
P cells
-
Color sensitive
-
Small receptive fields (finer resolution)
-
Slow, sustained
-
More sensitive at high contrast/ high spatial
frequency
-
Object Recognition! (infero-temporal
lobe)
Primary Visual Cortex (V1)
1st stop in cortex
-
Binocular integration (depth integration)
-
Computes simple features
Orientation
○
Ocular dominance
○
Spatial location
○
Colour
○
Spatial frequency
○
-
What is represented in striate cortex (V1)?
RF not spots of light as in LGN, but "bars" of light orientation
Simple cells prefer: orientation and location
§
Complex cells prefer: orientation
§
Hyper-complex cells prefer: orientation and length
§
○
-
How is V1 organized?
In orientation columns and ocular dominance columns in cortical layers
○
-
Visual organization
Neuronal preferences grow increasingly more complex
○
Receptive fields increase in size
TEO: posterior inferotemporal lobe
§
TE: anterior inferotemporal lobe
§
○
-
Object invariance: recognize object in different orientation
Dorsal stream (where) Ventral stream (what)
Medial superior temporal area &
middle temporal area
-
How? Lesion studies: Damage to
parietal lobe (dorsal stream) impair
spatial task (where)
-
Extrastriate and inferior temporal
-
How? Lesion studies: Damage to temporal lobe
(ventral stream) impairs object recognition
(what)
-
Blindsight
Cortical blindness
Extensive striate damage
○
-
Some of these patients show preservation of some visual discernment
But they have no awareness of "seeing"
○
-
V1 is necessary for conscious visual awareness
-
-
Dorsal visual stream (where)
Creates spatial map of the world
-
Track objects as they move
-
Spatial perception and action
-
Prepare for movement
-
Has LARGE receptive field
-
Damage
Optic Ataxia
Can recognize objects but cannot use info to guide action
§
Can see objects but cannot reach for them
§
○
-
Ventral visual stream (what)
Inferotemporal cortex
-
Process complex objects
-
Irrespective of orientation
-
Selectivity of objects
hands, tools, faces (strongest response -> weakest response)
○
-
Small receptive field at V1 (striate cortex) / large receptive field at IT
(inferotemporal cortex)
○
-
"what" object visual perception must solve problems of
Translation
○
Scale invariance
○
Orientation
○
Occlusion
○
Contrast variation
○
-
Testing invariance of recognition
Cue-from invariance
○
Perceptual constancy
○
Adaption (Repetition reduction)
○
Roles of Lateral occipital complex (LOC) in invariance
fMRI adaptation to same shape with different contour!
○
Damage
Apperceptive agnosia
Problem forming percepts
§
Can perceive parts, but not a meaningful whole
§
Cannot see integrated object
§
"I can’t see IT!"
§
○
Associate agnosia
Can perceive meaningful whole, but can’t link with knowledge
§
Problem accessing semantic info
§
Can see integrated object but don't know what it is
§
"I can see it, but I don't know what it is!"
§
○
-
Apperceptive agnosia Associate agnosia
Varying degrees of perceptual problems
(depend on lesion extent)
-
Deficit in copying form
-
Can’t perceive high-order visual structure
-
Can’t integrate parts into whole
-
Problem in object constancy
Viewing position •
Lighting •
Occlusion •
-
Damage in occipital lobe
-
Can copy complex objects but cannot
identify them
-
Perceptual grouping intact
-
Can copy objects but
Can't recall from memory •
Can’t match to function
But can match to visual
similarity
○
•
-
Damage in temporal lobe
-
The How pathway hypothesis
Patient D.F. - Apperceptive agnosia
Perception condition: Indicating using hand-held card - cannot put the card
○
Action condition: indicating by " posting in slot" - can put the card
○
-
She had damaged to her lateral occipital lobe in the what pathway (ventral), but her
where pathway (dorsal stream) is not damaged, which is the pathway for action. Thus
she cannot recognize the object but she can still perform the action.
-
Lesions to dorsal stream(where): optic ataxia (superior parietal lobe)
Inability to use visual info to reach out for objects located in the hemifield
contralateral to the lesion.
-
No difficulty recognizing objects that are presented in any part of the visual field
-
Lesion to ventral stream(what): visual agnosia
Inability to form a visual percept or link that percept the meaning
-
These patients often have no difficulty using vision to avoid obstacles
-
Double Dissociation:
Apperceptive agnosia (damage ventral) Optic ataxia (damage dorsal)
Impaired perception
-
Intact action
Appropriate reaching/grasping •
-
Intact perception
-
Impaired action
Eye: inappropriate saccades•
Hand: impaired reaching/grasping •
-
Perception (what) Action (how) Site of Damage
Apperceptive agnosia Ventral
Optic ataxia Dorsal
Special Agnosia: Prosopagnosia
Inability to perceive faces
-
Can perceive other objects though
-
Intact semantic info
-
Can process holistically, just not faces
-
Damage to FFA
-
Bilateral or right lesions
-
What does the face inversion effect tell us?
Face inversion effect: difficulty remembering/perceiving inverted relative to upright
faces
-
When upright: holistic/ configural processing of subtle relations b/w features
Overall configuration is critical for face identification and recognition
○
-
When inverted: local processing of features
Don’t notice configural violations
○
-
Prosopagnosics perform equivalently to controls on inverted faces
Impaired configural/holistic processing
○
Intact analytic/local processing
○
-
Fusiform Face Area (FFA)
Greeble experiment (face vs. expertise)
FFA and configural encoding
"greebles": part of greebles have fixed spatial relationships
§
All subjects began as novice recognizers
§
Train to recognize individuals
§
Evidence of configural processing
"greeble inversion effect"
Increased with training
®
□
§
As subjects gained expertise the "face area" of the brain responded more
strongly to "greebles" = evidence for plasticity
§
○
-
1. Evolutionary perspective
2. More active for faces than other configural objects
3. Prosopagnosics can differentiate configural objects but not faces
Selective areas in Extrastriate
-Fusiform face area (FFA)
-Extrastriate body area (EBA)
-Parahippocampal place area (PPA)
-Visual word form area (VWFA)
-Lateral occipital complex (LOC) - invariance
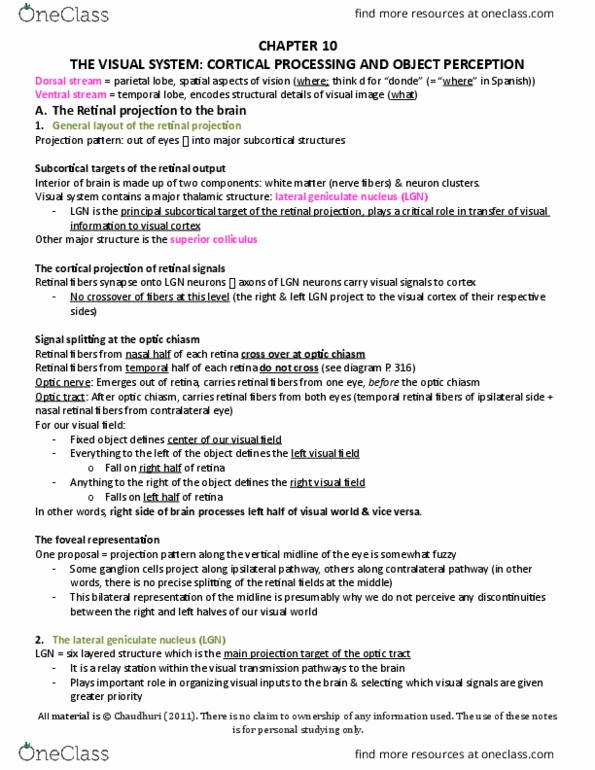
Photoreceptors
-
Image is inverted in retina
-
Left visual field
If lesion in area 2 then
black spot in your VF
area 2
Right visual cortex
Image projected in inverted fashion
Lecture 3
Friday, May 25, 2018 2:05 PM

Retina
Takes raw input of light (membrane polarization)
-
Light -> ganglion cells -> amacrine cell -> bipolar cell ->horizontal cell -> cone/rod
-
Photoreceptors: Rod & Cones
Light energy -> electrochemical energy
-
120 M rods vs. 6 M cones (more rods than cones)
Rods (abundant in retina)
Contain pigment Rhodopsin
§
Sensitive to small amount of light (in the dark)
§
Detect black, white and grey
§
Located in the periphery of the fovea
§
Many rods connect to one ganglion cell
§
○
Cones (sparse in retina)
3 different pigments called photopsins
Short wavelength -> blue □
Medium wavelength -> green□
Long wavelength -> Red □
§
Sensitive to large amount of light
§
Detect Color
§
Located at mostly at fovea
§
Few cones to ganglion (specificity)
§
○
-
Fovea
Huge concentration of cones
○
-
Rods vs. Cones
Rods are more useful at low light levels
Many rods to each ganglion cell = less resolution
§
○
Cones are better for detecting colour and detail
Few cones to each ganglion cell = more resolution
§
○
-
Receptive field
Area of space where a neuron maximally fires
-
Neuron is said to prefer a given stimulus
-
Also true for auditory, somatosensory systems
-
Center-surround Receptive Fields
Each cell has an excitatory and inhibitory area of sensitivity
-
On-center = activated
-
Off-center = deactivated
-
Ganglion cells (innervate the Lateral Geniculate Nucleus (LGN))
Some processing at the retina!
-
M cells (Parasol) -> magnocellular layer of LGN
Motion, B&W(rods), fast, large receptive fields!
○
-
P cells (Midget) -> parvocellular layer of LGN
Precise, colour (cones), slow, small receptive fields!
○
-
Visual pathways
Contralateral organization of visual pathways
-
Info from the right visual field is directed solely to the primary visual cortex (V1) on
the left hemisphere (left visual field to right hemisphere)
-
From Retina to Brain
Two main pathways
Tectopulvinar path
○
Geniculostriate path (LGN)
○
-
Tectopulvinar pathway
Retina -> superior colliculus -> pulvinar -> extrastriate cortex (V2)
Sensitive to motion and novelty
§
Contains 10% of optic nerves
§
Receives input from M cells
§
Sensitive to periphery, not fine detail
§
Automatic eye movement orientation
§
○
-
Geniculostriate pathway (LGN path)
Retina -> lateral geniculate nucleus 0 -> primary visual cortex (V1, striate
cortex)
Sensitive to colour and fine grained detail
§
Contains 90% of optic nerves
§
Receives input from M & P cells
§
○
-
LGN visual pathway
How does the brain convert sensory signals into the coherent objects we perceive?
Right nasal and right temporal -> left LGN
○
Left nasal and left temporal -> right LGN
○
-
Ipsilateral eye projects to layers 2, 3, 5
-
Contralateral eye to projects to layers 1, 4 and 6
-
Lateral Geniculate Nucleus (LGN)
Properties of LGN: Morphonogy
Not all retinal maps the same
○
M & P origins are maintained in LGN
Parvocellular layers
Receive input from midget ganglion cells (P cells) in the retina
Cone input predominates
®
□
Small cells □
Top 4 layers (3, 4, 5, 6)□
§
Magnocellular layers
Receive input from parasol ganglion cells (M cells) in the retina□
Large cells □
Bottom 2 layers (1, 2) □
§
○
-
Retinotopic Organization
Two paths within LGN
Magnocellular Pathway
Parvocellular pathway
M cells
-
Color insensitive
-
Large receptive fields
-
Fast, transient
-
More sensitve at low contrest/ low spatial
frequency
-
ACTION! (parietal lobe)
P cells
-
Color sensitive
-
Small receptive fields (finer resolution)
-
Slow, sustained
-
More sensitive at high contrast/ high spatial
frequency
-
Object Recognition! (infero-temporal
lobe)
Primary Visual Cortex (V1)
1st stop in cortex
-
Binocular integration (depth integration)
-
Computes simple features
Orientation
○
Ocular dominance
○
Spatial location
○
Colour
○
Spatial frequency
○
-
What is represented in striate cortex (V1)?
RF not spots of light as in LGN, but "bars" of light orientation
Simple cells prefer: orientation and location
§
Complex cells prefer: orientation
§
Hyper-complex cells prefer: orientation and length
§
○
-
How is V1 organized?
In orientation columns and ocular dominance columns in cortical layers
○
-
Visual organization
Neuronal preferences grow increasingly more complex
○
Receptive fields increase in size
TEO: posterior inferotemporal lobe
§
TE: anterior inferotemporal lobe
§
○
-
Object invariance: recognize object in different orientation
Dorsal stream (where) Ventral stream (what)
Medial superior temporal area &
middle temporal area
-
How? Lesion studies: Damage to
parietal lobe (dorsal stream) impair
spatial task (where)
-
Extrastriate and inferior temporal
-
How? Lesion studies: Damage to temporal lobe
(ventral stream) impairs object recognition
(what)
-
Blindsight
Cortical blindness
Extensive striate damage
○
-
Some of these patients show preservation of some visual discernment
But they have no awareness of "seeing"
○
-
V1 is necessary for conscious visual awareness
-
-
Dorsal visual stream (where)
Creates spatial map of the world
-
Track objects as they move
-
Spatial perception and action
-
Prepare for movement
-
Has LARGE receptive field
-
Damage
Optic Ataxia
Can recognize objects but cannot use info to guide action
§
Can see objects but cannot reach for them
§
○
-
Ventral visual stream (what)
Inferotemporal cortex
-
Process complex objects
-
Irrespective of orientation
-
Selectivity of objects
hands, tools, faces (strongest response -> weakest response)
○
-
Small receptive field at V1 (striate cortex) / large receptive field at IT
(inferotemporal cortex)
○
-
"what" object visual perception must solve problems of
Translation
○
Scale invariance
○
Orientation
○
Occlusion
○
Contrast variation
○
-
Testing invariance of recognition
Cue-from invariance
○
Perceptual constancy
○
Adaption (Repetition reduction)
○
Roles of Lateral occipital complex (LOC) in invariance
fMRI adaptation to same shape with different contour!
○
Damage
Apperceptive agnosia
Problem forming percepts
§
Can perceive parts, but not a meaningful whole
§
Cannot see integrated object
§
"I can’t see IT!"
§
○
Associate agnosia
Can perceive meaningful whole, but can’t link with knowledge
§
Problem accessing semantic info
§
Can see integrated object but don't know what it is
§
"I can see it, but I don't know what it is!"
§
○
-
Apperceptive agnosia Associate agnosia
Varying degrees of perceptual problems
(depend on lesion extent)
-
Deficit in copying form
-
Can’t perceive high-order visual structure
-
Can’t integrate parts into whole
-
Problem in object constancy
Viewing position •
Lighting •
Occlusion •
-
Damage in occipital lobe
-
Can copy complex objects but cannot
identify them
-
Perceptual grouping intact
-
Can copy objects but
Can't recall from memory •
Can’t match to function
But can match to visual
similarity
○
•
-
Damage in temporal lobe
-
The How pathway hypothesis
Patient D.F. - Apperceptive agnosia
Perception condition: Indicating using hand-held card - cannot put the card
○
Action condition: indicating by " posting in slot" - can put the card
○
-
She had damaged to her lateral occipital lobe in the what pathway (ventral), but her
where pathway (dorsal stream) is not damaged, which is the pathway for action. Thus
she cannot recognize the object but she can still perform the action.
-
Lesions to dorsal stream(where): optic ataxia (superior parietal lobe)
Inability to use visual info to reach out for objects located in the hemifield
contralateral to the lesion.
-
No difficulty recognizing objects that are presented in any part of the visual field
-
Lesion to ventral stream(what): visual agnosia
Inability to form a visual percept or link that percept the meaning
-
These patients often have no difficulty using vision to avoid obstacles
-
Double Dissociation:
Apperceptive agnosia (damage ventral) Optic ataxia (damage dorsal)
Impaired perception
-
Intact action
Appropriate reaching/grasping •
-
Intact perception
-
Impaired action
Eye: inappropriate saccades•
Hand: impaired reaching/grasping •
-
Perception (what) Action (how) Site of Damage
Apperceptive agnosia Ventral
Optic ataxia Dorsal
Special Agnosia: Prosopagnosia
Inability to perceive faces
-
Can perceive other objects though
-
Intact semantic info
-
Can process holistically, just not faces
-
Damage to FFA
-
Bilateral or right lesions
-
What does the face inversion effect tell us?
Face inversion effect: difficulty remembering/perceiving inverted relative to upright
faces
-
When upright: holistic/ configural processing of subtle relations b/w features
Overall configuration is critical for face identification and recognition
○
-
When inverted: local processing of features
Don’t notice configural violations
○
-
Prosopagnosics perform equivalently to controls on inverted faces
Impaired configural/holistic processing
○
Intact analytic/local processing
○
-
Fusiform Face Area (FFA)
Greeble experiment (face vs. expertise)
FFA and configural encoding
"greebles": part of greebles have fixed spatial relationships
§
All subjects began as novice recognizers
§
Train to recognize individuals
§
Evidence of configural processing
"greeble inversion effect"
Increased with training
®
□
§
As subjects gained expertise the "face area" of the brain responded more
strongly to "greebles" = evidence for plasticity
§
○
-
1. Evolutionary perspective
2. More active for faces than other configural objects
3. Prosopagnosics can differentiate configural objects but not faces
Selective areas in Extrastriate
-Fusiform face area (FFA)
-Extrastriate body area (EBA)
-Parahippocampal place area (PPA)
-Visual word form area (VWFA)
-Lateral occipital complex (LOC) - invariance
Photoreceptors
-
Image is inverted in retina
-
Left visual field
If lesion in area 2 then
black spot in your VF
area 2
Right visual cortex
Image projected in inverted fashion
Lecture 3
Friday, May 25, 2018 2:05 PM
Document Summary
Right nasal and right temporal -> left lgn. Left nasal and left temporal -> right lgn. Ipsilateral eye projects to layers 2, 3, 5. Contralateral eye to projects to layers 1, 4 and 6. M & p origins are maintained in lgn. Receive input from midget ganglion cells (p cells) in the retina. Receive input from parasol ganglion cells (m cells) in the retina. If lesion in area 2 then black spot in your vf area 2. More sensitve at low contrest/ low spatial frequency. More sensitive at high contrast/ high spatial frequency. Rf not spots of light as in lgn, but bars of light orientation. In orientation columns and ocular dominance columns in cortical layers. Medial superior temporal area & middle temporal area. Lesion studies: damage to parietal lobe (dorsal stream) impair spatial task (where) Lesion studies: damage to temporal lobe (ventral stream) impairs object recognition (what) Some of these patients show preservation of some visual discernment.