Physiology 3120 Lecture 3: Renal

9 May 2018
School
Department
Course
Professor

Physiology 3120
Dr. Woods
Lecture 3
Filtration Coefficient
- There are layers of tissues which will affect your filtration rate
- The NFP is the biggest contributor to your GFR (rate of fluid we filter per day)
- Within those pressures, the hydrostatic pressure of glomerular capillaries (the fact htat blood is
pumping through your nephrons at a pressure bc of your heart) – that is the biggest thing
affecting NFP
- But we have other things that can affect it
o Ex: surface area
▪ in the corpuscle, we have glomerular capillaries that sit in the corpuscle and has
surface area available for filtration (this area that is available is the slits bw the
podocytes)
▪ SO the size of the slits bw the podocytes is the area available for fluid flow
o Ex: basal lamina
▪ Barrier that removes the opportunity for proteins and other things to get out of
the blood
▪ The barrier can also change filtration n
▪ If you change the permeability of the basal lamina, you will also affect the fluid
flow rate not just the exclusion of proteins
▪ If the basal lamina became less permeable due to for ex scar tissue, your barrier
would be less permeable and so less fluid can flow in
▪ If the basal lamina were destructed or you had a mutation that affected the
integrity of the collagen that made it thinner, you would change the fluid flow
rate
▪ This may also cause you to possibly start leaking proteins as well
- Net filtration pressures mostly contribute to the GFR
- But surface area available for filtration and permeability of barriers can contribute to the GFR
- What would be the consequence of the following:
1. Increasing space between podocytes
o Rate of things that were already able to pass through increases
o Increased fluid flow rate
o If you totally remove the podocytes, then you might start leaking other things
2. Increasing the permeability of the basal lamina
o The fluid flow rate increases
o You also change the things that are being filtered (proteins could get through)
3. Decreasing the size of the glomerular pores
o You decrease fluid flow rate
o )t doesn’t change that much
GFR Regulation by Renal Blood Flow
- Changing the diameters of the afferent and efferent arteriole will affect the hydrostatic pressure
in the glomerulus which will regulate fluid flow rate
- What would happen to the pressure in the glomerulus if the following occurred:
o Afferent arteriole constricted
▪ Renal blood flow will decreasepressure decreases decrease GFR
o Efferent arteriole constricted
▪ Renal blood flow will increase pressure increases increase GFR
o Both arterioles constricted
▪ Depending on the magnitude of the constriction, renal blood flow will differ
find more resources at oneclass.com
find more resources at oneclass.com

▪ If it was a slight constriction, it might balance each other out
▪ Angiotensin II potent vasoconstrictor that constricts both afferent and
efferent arterioles (highly constricts the arterioles) renal blood flow will
decrease pressure decreases decrease GFR
Autoregulation of GFR
- This regulation is happening on its own – you don’t have to control this there are no hormones
controlling this)
- However, we do have other mechanisms that use hormones to regulate GFR
- 2 autoregulator responses:
o myogenic response
o tubuloglomerular feedback
Myogenic Response
- When blood pressure increases:
o afferent arteriole stretches stretch sensitive cation channels open within the vascular
smooth muscle smooth muscle cells in the afferent arteriole depolarizevoltage-
gated calcium channels open in smooth muscle (Ca2+ flows in)smooth muscle
contracts (afferent arteriole constricts) blood flow decreases in the glomerulus
- we want that blood pressure to stay low
- its not just that we want to maintain GFR its also a protective mechanism
- the glomerular capillaries are a very delicate tissue so we don’t want it to experience pressure
that is too high bc those glomerular capillaries could rupture and we don’t have great
regenerative capacity in our nephrons
- so its alos a protective mechanism to keep nephrons functioning properly
Tubuloglomerular Feedback
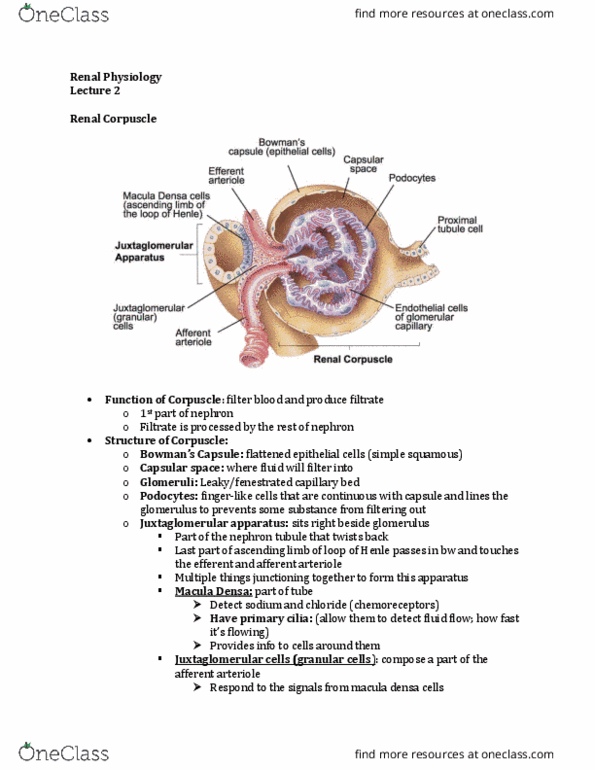
- JGA is the last part of the ascending limb of the loop of henle that physically touches the
corpuscle in bw the afferent and efferent corpuscle
- We also have macula densa cells within this junction
- Note: there is not that many macula densa cells (10-20 of these cells
are macula densa cells) – responsible for detecting fluid composition
they send signal to the juxtaglomerular cells (granular cells) which
are modified smooth muscle cells on the afferent arteriole
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
There are layers of tissues which will affect your filtration rate. The nfp is the biggest contributor to your gfr (rate of fluid we filter per day) Within those pressures, the hydrostatic pressure of glomerular capillaries (the fact htat blood is pumping through your nephrons at a pressure bc of your heart) that is the biggest thing. If you change the permeability of the basal lamina, you will also affect the fluid flow rate not just the exclusion of proteins. If the basal lamina became less permeable due to for ex scar tissue, your barrier would be less permeable and so less fluid can flow in. Net filtration pressures mostly contribute to the gfr. But surface area available for filtration and permeability of barriers can contribute to the gfr. What would be the consequence of the following: Increasing space between podocytes: rate of things that were already able to pass through increases.