NURS 443 Lecture Notes - Lecture 12: Dysphonia, Interferon, Balsalazide


Immunity
Book Notes
A. Tuberculosis (TB)
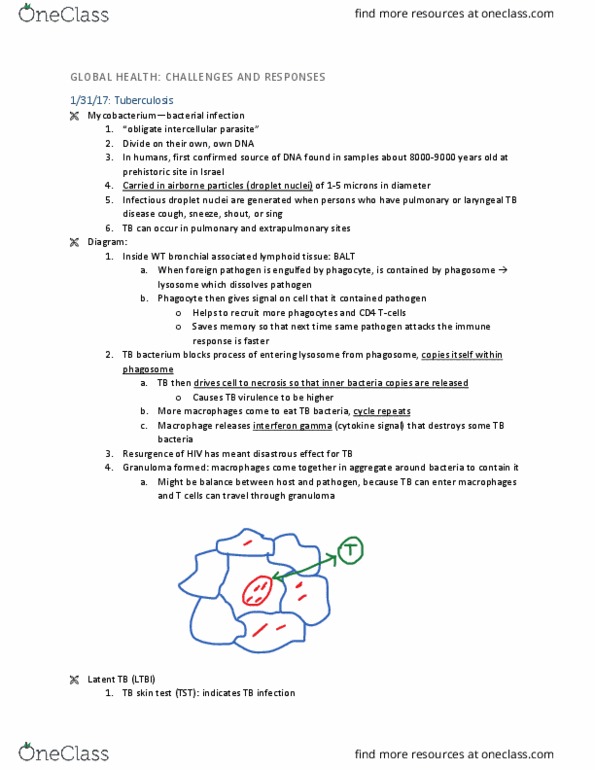
1. Patho: infectious disease caused by Mycobacterium tuberculosis that spreads through
airborne droplet. Typically involves the lungs but can affect any organ.
a. Leading cause of death in HIV pts.
b. Once it develops resistance to (isoniazid or rifampin) than it is considered multi-drug
resistant tuberculosis (MDR-TB)
c. Three TB- related conditions: latent TB Infection (LTBI), Primary, and Active TB
disease
i. Primary is when bacteria is inhaled but immune response occurs and bacteria
becomes inactive
ii. Latent will not have symptoms and cannot infect others: typical in HIV or
immunosuppressed pts.
iii. Active occurs when initial immune response is not adequate, the body cannot
contain the organism, and the bacteria replicates.
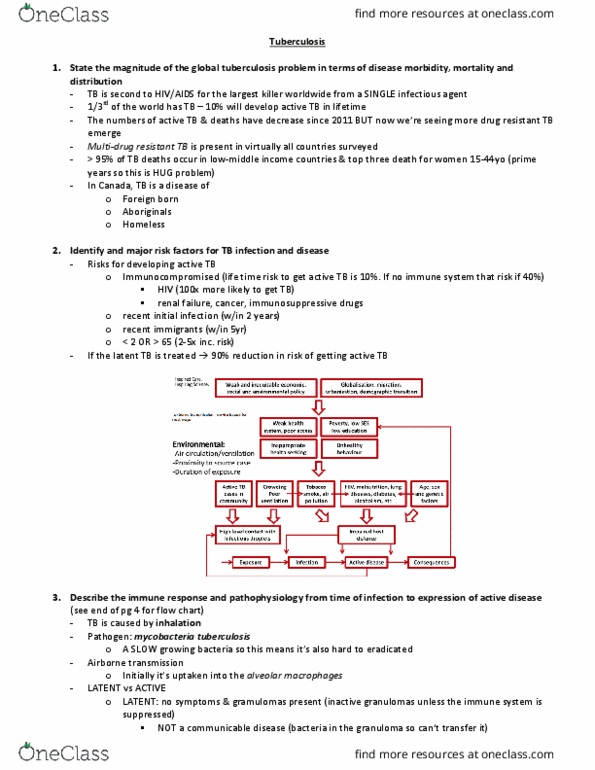
2. Risks:
a. homeless, foreign-born ppl, inner-city neighborhoods, living or working in
institutions, IV injecting drug users, immunosuppression or HIV, Asian decent
3. Cause:
a. M. tuberculosis spread through airborne droplets from breathing, talking, singing,
sneezing, and coughing
b. Factors that influence transmission: (1) number of organisms expelled in air, (2)
concentration of organisms, (3) length of time of exposure, (4) immune system of
the exposed person
c. CANNOT be spread: touching, sharing utensils, kissing, or other physical contact
4. Classification (table 28-8 pg. 529)
a. 0: No TB exposure
b. 1: TB exposure, no infection
c. 2: latent TB infection, no disease
d. 3: TB, clinically active
e. 4: TB, not clinical active
f. 5: TB suspect
5. S&S
a. If latent TB: positive skin test but are asymptomatic
b. If puloar TB: sptos tpiall do’t deelop util 2-3 wks after infection.
i. Initial dry cough that frequently becomes productive w/ mucoid or
mucopurulent sputum, hemoptysis, chest pain, anorexia, weight loss, night
sweats, fever, fatigue
c. If extrapulmonary TB
i. Depends on body system
1. Kidney (hematuria), Meninges (headache and confusion), Spine (back
pain), Larynx (hoarseness)
d. If active TB: may initially manifest w/ constitutional symptoms such as fatigue,
malaise, anorexia, unexplained weight loss, low-grade fever, and night sweats.
i. Dyspnea is late sympt. That indicates pleural effusion
e. At times it could be sudden high fever, chills, generalized flu-like symptoms, pleuritic
pain, and productive cough
find more resources at oneclass.com
find more resources at oneclass.com

f. Immunosuppressed or elderly
i. Elderly may not have fever and other signs of infection
ii. HIV may show fever, cough, and weight loss but may be confused with
another HIV associated disease.
6. Complications
a. Miliary TB- widespread dissemination of M. tuberculosis. Can be fatal if left
untreated.
b. Acute pneumonia my result when large amounts of tubercle bacilli are discharged
from granulomas in lungs
7. Diagnosis
a. Gold Standard for CONFIRMATION of TB disease is AFB (acid fast bacillus) smear and
culture
i. If negative it does not necessary exclude TB disease
b. Tuberculin skin test (TST) is the standard method for SCREENING
i. Injection of PPD intradermally on forearm and w/I 48-72 hrs will be read.
1. Induration (no redness) means person has been exposed to TB and has
developed antibodies which occurs 2-12 wks after exposure
c. Interferon- Release Assa IGRA’s
i. Only require one visit, not subject to reader bias, have no booster
phenomenon, and are not affected by prior bacillus Calmette.
d. Chest X-Ray
i. Diagnosis cannot be based only on x-ray because other diseases may mimic
TB
8. Treatment
a. Pharmacological (table 28-11 pg. 531)
i. Active treatment: Can either be initial and continuation medication (Table 28-
11 pg. 531)
a. Typically a 6-9 month, four-drug therapy.
2. Isoniazid (INH)
a. SE: hepatitis, asympt. Elevation of aminotransferases (ALT/AST)
b. Monitor liver function tests monthly (before, during, and after
taking drug), alcohol can increase hepatotoxicity
3. Rifampin (RIfadin) or rifabutin (Mycobutin)
a. SE: hepatitis, thrombocytopenia, orange discoloration of body
fluids
4. Pyrazinamide: hepatitis, arthralgias, hyperuricemia
5. Ethambutol
a. SE: ocular toxicity (decreased red-green color discrimination)
b. Monitor visual acuity and color discrimination
6. Streptomycin
a. SE: dysrhythmias, oto/nephro toxicity
ii. If MDR TB
1. Typically diagnosed if they do not respond to isoniazid or rifampin
2. Etesie if the do’t respod to isoiazid, rifapi, a
fluroquinolone and at least one of the 3 injectable second-line drugs
iii. Latent treatment: (Table 28-13 pg. 532)
1. Typically 9 mnths daily dosage of INH
9. Interventions
find more resources at oneclass.com
find more resources at oneclass.com

a. In order to be non-infectious
i. Must have three consecutive negative AFB smears collected at 8-24 hr
intervals
ii. Clinical improvement of symptoms
iii. Compliance w/ treatment regimen for 2 wks or longer
b. Vaccine BCG is live and typically not given to infants in the US but can be given to
infants in other parts of the world or those exposed to MDR-TB.
c. Screen any individuals that had close contact with the pt.
d. Restrict visitors and avoid travel on public transportation/ trips to public places
e. Place in airborne isolation and in negative pressure room, receive a medical workup;
chest X-Ray/sputum smear/ and culture, & receive appropriate drug therapy
f. HEPA mask should be worn when entering pts. Room ad should e fit tested
g. Encourage pt. to cover mouth with paper tissue when coughing, sneezing, or
spitting out sputum. The tissue should then be thrown into a paper bag and
disposed w/ trash/ burned/ or flushed down the toilet.
h. If pt. leaves the room they must wear standard isolation masks to prevent exposure
to others
10. Ambulatory/ Home care
a. Keep a strict adherence to prescribed medications. Strategies to improve include;
reminder systems (spouse, pill boxes, etc), incentive or rewards, contracts, and DOT
(directly observed treatment/ watch pt. swallow medication)
b. Monthly sputum cultures are obtained until two consecutive specimens are (-)
c. Pt. should sleep alone, spend time outdoors, and minimize time in congregate
settings
d. Public health department must be notified.
e. Pt. should be encourage to quit smoking
B. Anaphylaxis
1. Patho: hypersensitive reaction after exposure to offending allergen.
2. Cause (Table 14-9 pg. 211)
a. Parenteral injection of drugs, blood products, or insect stings.
b. Hypovolemic shock because of loss in intravascular fluid into interstitial spaces
3. S&S (Table 14-7 pg. 211)
a. Sudden reaction of edema and itching at site of exposure. Rapid, weak pulse;
hypotension; dilated pupils; dyspnea; cyanosis
4. Interventions
a. Put ALL of pts. Allergies in medical record
b. Recognize S&S of anaphylactic reaction
c. maintenance of patent airway
d. prevent spread of allergen by using a tourniquet
e. admit of dugs/ treatment for shock
C. Inflammatory Bowel Disease (IBD)
1. Patho: an autoimmune disease in which chronic inflammation of the GI tract occurs
a. Characterized by periods of remission interspersed w/ periods of exacerbation
b. Unknown cause and no cure
c. Classified as either Croh’s or Uleratie olitis
2. Risks: genetics (NOD2), diet (fatty meats, Omega-6 fatty acids), hygiene, stress, smoking,
increased NSAID use, Caucasian race (especially jewish).
3. Complications: (table 43-15 pg. 977)
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Book notes: patho: infectious disease caused by mycobacterium tuberculosis that spreads through airborne droplet. Can be fatal if left untreated: acute pneumonia my result when large amounts of tubercle bacilli are discharged from granulomas in lungs, diagnosis, gold standard for confirmation of tb disease is afb (acid fast bacillus) smear and culture. If negative it does not necessary exclude tb disease: tuberculin skin test (tst) is the standard method for screening. Injection of ppd intradermally on forearm and w/i 48-72 hrs will be read. 531: active treatment: can either be initial and continuation medication (table 28- Elevation of aminotransferases (alt/ast: monitor liver function tests monthly (before, during, and after taking drug), alcohol can increase hepatotoxicity, rifampin (rifadin) or rifabutin (mycobutin) Se: hepatitis, thrombocytopenia, orange discoloration of body fluids: pyrazinamide: hepatitis, arthralgias, hyperuricemia, ethambutol. Se: ocular toxicity (decreased red-green color discrimination: monitor visual acuity and color discrimination, streptomycin. 532: typically 9 mnths daily dosage of inh.