ESS 150 Lecture Notes - Lecture 9: Fibular Collateral Ligament, Medial Meniscus, Sprain

30 Apr 2018
School
Department
Course
Professor

Special Tests for Knee Stability
Compare injured knee to uninjured knee
-
Valgus/ Varus stress test
Used to reveal laxity (鬆弛) of the MCL and LCL
○
Valgus force moves lateral to medial (test MCL)
○
Varus force moves medial to lateral (test LCL)
○
-
Genus valgum
Knock-knee
-
A condition in which the knees angle in and can touch one another when legs
are straightened
-
Knees turn
-
-
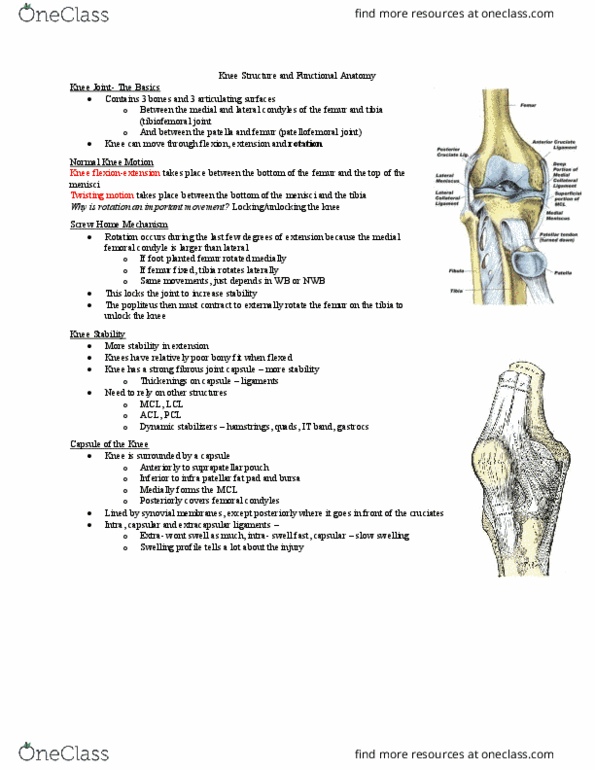
Ligament Injuries
Major ligaments of the knee can be torn in isolation or in combination
-
Injury can result from direct line force, rotary force or combination of the two
-
Medial Collateral Ligament Sprain
Cause of injury
Result of severe blow or outward twist- valgus force
○
-
Signs of injury- Grade I
Little fiber tearing or stretching
○
Stable valgus test
○
Little or no joint effusion
○
Some joint stiffness and point tenderness on lateral aspect
○
Relatively normal ROM
○
-
Signs of injury- Grade II
Complete tear of deep capsule ligament and partial tear of superficial
layer of MCL
○
No gross instability; slight laxity
○
Slight swelling
○
Moderate to severe joint tightness with decreased ROM
○
Pain along medial aspect of knee
○
-
Signs of injury- Grade III
Complete tear of supporting ligaments
○
Complete loss of medial stability, meniscus disruption
○
Minimum to moderate swelling
○
Immediate pain followed by ache
○
Loss of motion due to effusion and hamstring
○
-
Care
RICE for at least 24 hours
○
Crutches if necessary
○
Knee immobilizer may be applied
○
Move from isometrics and STLR exercises to bicycle riding and isokinetic
○
Return to play when all areas have returned to normal
Continued bracing may be required
§
○
-
Lateral collateral ligament sprain
Cause of injury
Result of a Varus force, generally with the fibula internally rotated
○
Direct blow is rare
○
-
Sign of injury
Pain and tenderness over LCL
○
Swelling and effusion around the LCL
○
Joint laxity with Varus testing
○
-
Care
Following management of MCL collateral ligament sprain
○
-
Anterior Cruciate Ligament Sprain
Cause: fairly common
MOI: athlete decelerates with foot planted and turns in the direction of
the planted foot forcing tibia into internal rotation
○
May be linked to inability to decelerate valgus and rotational stresses-
landing strategies
○
Male versus female injury rates
More common in female
Due to hormonal, anatomy, conditioning?□
biomechanics most likely □
§
○
Impact of femoral notch, ACL size and laxity, malalignment (Q-angle)
faulty biomechanics
○
Extrinsic factors may include, conditioning, skill acquisition, playing style,
equipment, preparation time
○
Also involve damage to other structures including meniscus, capsule, MCL
○
-
Sign
Experience pop with severe pain and disability
○
Positive anterior drawer and Lachman's
○
Rapid swelling at the joint line
○
-
Care
RICE, use of crutches
○
Arthroscopy may be necessary to determine extent of injury
○
Could lead to major instability in incidence of high performance
○
Without surgery joint degeneration may result
○
Age and activity may factor into surgical option
○
** can take a long time to heal**
○
Surgery may involve joint reconstruction with grafts (tendon)
transplantation of external structures
Will require brief hospital stay and 3-5 weeks of a race
§
Also requires 4-6 months of rehab
§
○
-
Lachman's Test
Most commonly used test for integrity of ACL
-
At 30 degrees of flexion attempt is made to translate the tibia anteriorly on the
femur
-
When it ACL is inflamed, it may show a smaller rotation
-
Posterior Cruciate Ligament Sprain
Cause of injury
Most at risk during 90 degree of flexion
○
Fail on bent knee is most common mechanism
○
Can also be damaged as a result of a rotational force
○
-
Sign
Feel a pop in the back of the knee
○
Tenderness and swelling in the popliteal fossa
○
Laxity with posterior sag test
○
-
Care
RICE
○
Non-operative rehab of grade I and II injuries should focus quad strength
○
Surgical versus non-operative care
○
-
PCL test- Posterior Drawer test
Meniscus Injuries
Cause
Medial meniscus is more commonly injured due to ligamentous
attachments and decreased mobility
Also more prone to disruption through torsional and valgus force
§
○
Result from weight bearing combined with rotation
○
-
Sign
Diagnosis is difficult
○
Effusion developing over 48-72 hour period
○
Joint line pain and loss of motion
○
Intermittent locking and giving way
○
Pain with squatting
○
-
CARE
Immediate care= PRICE
○
If the knee isn't locked, but indications of a tear are present further
diagnostic testing may be required
Treatment should follow that of MCL injury
§
○
If locking occurs, anesthesia may be necessary to unlock the joint with
possible arthroscopic surgery follow- up
○
-
Apley's compression test
Used to detect meniscus tear
-
Knee at 90 degree apply hard downward pressure with rotation
-
Pain indicates meniscal injury
-
Medial tear- external rotation
-
Lateral tear- internal rotation
-
Joint contusions (bruises)
Cause of injury
Blow to the muscles crossing the joint (varstus medial - quadriceps)
○
-
Sign
Present as knee sprain, severe pain, loss of movement and signs of acute
inflammation
○
Swelling
○
-
Knee plica
Plica: a thickened fold of synovial membrane lining the inside of the joint
capsule. 3 of them around the knee joint infra, supra, mediopatellar plica)
-
Cause
Mechanism of injury
Twisting knee with foot fixed sitting for long period of time
§
○
-
Bursitis
Cause
Acute, chronic or recurrent swelling
○
Prepatellar= contused kneeing
○
Infrapatellar= overuse of patellar tendon
○
-
Sign
Prepatellar bursitis may be localized swelling above knee that is similar to
a balloon
○
Presents with signs of inflammation (swelling, redness)
○
Swelling in back of the knee may indicate
○
-
Loose bodies (joint mice)
Cause
Result of repeated trauma
○
Possibly stems from fragments of bone or meniscal fragments, synovial
tissue or cruciate ligaments
○
-
Sign
May become lodged, causing locking or popping
○
Pain and sensation of instability
○
-
Care
If not surgically removed, it can lead to conditions causing joint
degeneration
○
-
Iliotibial band friction syndrome
"runner's knee"
-
Cause
Repetitive/ overuse conditions attributed to mal-alignment and structural
asymmetries
○
Result of repeated knee flexion and extension
○
-
Sign
Irritation at band's insertion (lateral side of the knee)
○
pain with activity
○
-
Care
Avoidance of aggravating activities
○
Correction of mal-alignments
○
Ice before and after activity, proper warm-up and stretching
○
-
Fracture of patella
Cause
Direct or indirect trauma (severe pull of tendon)
○
Forcible contraction, falling, jumping or running
○
-
Sign
Hemorrhaging with generalized swelling
○
Little bone separation with direct injury (fragments)
○
Indirect fractures may cause joint capsular tearing, separation of bone
fragments and possible quadricep tendon tearing
○
-
Management
X-ray is needed because it's a bone injury
○
Refer and immobilize for 2-3 months
○
-
-
Lecture 9
Wednesday, April 25, 2018
9:03 AM

Special Tests for Knee Stability
Compare injured knee to uninjured knee
-
Valgus/ Varus stress test
Used to reveal laxity (鬆弛) of the MCL and LCL
○
Valgus force moves lateral to medial (test MCL)
○
Varus force moves medial to lateral (test LCL)
○
-
Genus valgum
Knock-knee
-
A condition in which the knees angle in and can touch one another when legs
are straightened
-
Knees turn
-
-
Ligament Injuries
Major ligaments of the knee can be torn in isolation or in combination
-
Injury can result from direct line force, rotary force or combination of the two
-
Medial Collateral Ligament Sprain
Cause of injury
Result of severe blow or outward twist- valgus force
○
-
Signs of injury- Grade I
Little fiber tearing or stretching
○
Stable valgus test
○
Little or no joint effusion
○
Some joint stiffness and point tenderness on lateral aspect
○
Relatively normal ROM
○
-
Signs of injury- Grade II
Complete tear of deep capsule ligament and partial tear of superficial
layer of MCL
○
No gross instability; slight laxity
○
Slight swelling
○
Moderate to severe joint tightness with decreased ROM
○
Pain along medial aspect of knee
○
-
Signs of injury- Grade III
Complete tear of supporting ligaments
○
Complete loss of medial stability, meniscus disruption
○
Minimum to moderate swelling
○
Immediate pain followed by ache
○
Loss of motion due to effusion and hamstring
○
-
Care
RICE for at least 24 hours
○
Crutches if necessary
○
Knee immobilizer may be applied
○
Move from isometrics and STLR exercises to bicycle riding and isokinetic
○
Return to play when all areas have returned to normal
Continued bracing may be required
§
○
-
Lateral collateral ligament sprain
Cause of injury
Result of a Varus force, generally with the fibula internally rotated
○
Direct blow is rare
○
-
Sign of injury
Pain and tenderness over LCL
○
Swelling and effusion around the LCL
○
Joint laxity with Varus testing
○
-
Care
Following management of MCL collateral ligament sprain
○
-
Anterior Cruciate Ligament Sprain
Cause: fairly common
MOI: athlete decelerates with foot planted and turns in the direction of
the planted foot forcing tibia into internal rotation
○
May be linked to inability to decelerate valgus and rotational stresses-
landing strategies
○
Male versus female injury rates
More common in female
Due to hormonal, anatomy, conditioning?□
biomechanics most likely □
§
○
Impact of femoral notch, ACL size and laxity, malalignment (Q-angle)
faulty biomechanics
○
Extrinsic factors may include, conditioning, skill acquisition, playing style,
equipment, preparation time
○
Also involve damage to other structures including meniscus, capsule, MCL
○
-
Sign
Experience pop with severe pain and disability
○
Positive anterior drawer and Lachman's
○
Rapid swelling at the joint line
○
-
Care
RICE, use of crutches
○
Arthroscopy may be necessary to determine extent of injury
○
Could lead to major instability in incidence of high performance
○
Without surgery joint degeneration may result
○
Age and activity may factor into surgical option
○
** can take a long time to heal**
○
Surgery may involve joint reconstruction with grafts (tendon)
transplantation of external structures
Will require brief hospital stay and 3-5 weeks of a race
§
Also requires 4-6 months of rehab
§
○
-
Lachman's Test
Most commonly used test for integrity of ACL
-
At 30 degrees of flexion attempt is made to translate the tibia anteriorly on the
femur
-
When it ACL is inflamed, it may show a smaller rotation
-
Posterior Cruciate Ligament Sprain
Cause of injury
Most at risk during 90 degree of flexion
○
Fail on bent knee is most common mechanism
○
Can also be damaged as a result of a rotational force
○
-
Sign
Feel a pop in the back of the knee
○
Tenderness and swelling in the popliteal fossa
○
Laxity with posterior sag test
○
-
Care
RICE
○
Non-operative rehab of grade I and II injuries should focus quad strength
○
Surgical versus non-operative care
○
-
PCL test- Posterior Drawer test
Meniscus Injuries
Cause
Medial meniscus is more commonly injured due to ligamentous
attachments and decreased mobility
Also more prone to disruption through torsional and valgus force
§
○
Result from weight bearing combined with rotation
○
-
Sign
Diagnosis is difficult
○
Effusion developing over 48-72 hour period
○
Joint line pain and loss of motion
○
Intermittent locking and giving way
○
Pain with squatting
○
-
CARE
Immediate care= PRICE
○
If the knee isn't locked, but indications of a tear are present further
diagnostic testing may be required
Treatment should follow that of MCL injury
§
○
If locking occurs, anesthesia may be necessary to unlock the joint with
possible arthroscopic surgery follow- up
○
-
Apley's compression test
Used to detect meniscus tear
-
Knee at 90 degree apply hard downward pressure with rotation
-
Pain indicates meniscal injury
-
Medial tear- external rotation
-
Lateral tear- internal rotation
-
Joint contusions (bruises)
Cause of injury
Blow to the muscles crossing the joint (varstus medial - quadriceps)
○
-
Sign
Present as knee sprain, severe pain, loss of movement and signs of acute
inflammation
○
Swelling
○
-
Knee plica
Plica: a thickened fold of synovial membrane lining the inside of the joint
capsule. 3 of them around the knee joint infra, supra, mediopatellar plica)
-
Cause
Mechanism of injury
Twisting knee with foot fixed sitting for long period of time
§
○
-
Bursitis
Cause
Acute, chronic or recurrent swelling
○
Prepatellar= contused kneeing
○
Infrapatellar= overuse of patellar tendon
○
-
Sign
Prepatellar bursitis may be localized swelling above knee that is similar to
a balloon
○
Presents with signs of inflammation (swelling, redness)
○
Swelling in back of the knee may indicate
○
-
Loose bodies (joint mice)
Cause
Result of repeated trauma
○
Possibly stems from fragments of bone or meniscal fragments, synovial
tissue or cruciate ligaments
○
-
Sign
May become lodged, causing locking or popping
○
Pain and sensation of instability
○
-
Care
If not surgically removed, it can lead to conditions causing joint
degeneration
○
-
Iliotibial band friction syndrome
"runner's knee"
-
Cause
Repetitive/ overuse conditions attributed to mal-alignment and structural
asymmetries
○
Result of repeated knee flexion and extension
○
-
Sign
Irritation at band's insertion (lateral side of the knee)
○
pain with activity
○
-
Care
Avoidance of aggravating activities
○
Correction of mal-alignments
○
Ice before and after activity, proper warm-up and stretching
○
-
Fracture of patella
Cause
Direct or indirect trauma (severe pull of tendon)
○
Forcible contraction, falling, jumping or running
○
-
Sign
Hemorrhaging with generalized swelling
○
Little bone separation with direct injury (fragments)
○
Indirect fractures may cause joint capsular tearing, separation of bone
fragments and possible quadricep tendon tearing
○
-
Management
X-ray is needed because it's a bone injury
○
Refer and immobilize for 2-3 months
○
-
-
Lecture 9
Wednesday, April 25, 2018
9:03 AM

Special Tests for Knee Stability
Compare injured knee to uninjured knee
-
Valgus/ Varus stress test
Used to reveal laxity (鬆弛) of the MCL and LCL
○
Valgus force moves lateral to medial (test MCL)
○
Varus force moves medial to lateral (test LCL)
○
-
Genus valgum
Knock-knee
-
A condition in which the knees angle in and can touch one another when legs
are straightened
-
Knees turn
-
-
Ligament Injuries
Major ligaments of the knee can be torn in isolation or in combination
-
Injury can result from direct line force, rotary force or combination of the two
-
Medial Collateral Ligament Sprain
Cause of injury
Result of severe blow or outward twist- valgus force
○
-
Signs of injury- Grade I
Little fiber tearing or stretching
○
Stable valgus test
○
Little or no joint effusion
○
Some joint stiffness and point tenderness on lateral aspect
○
Relatively normal ROM
○
-
Signs of injury- Grade II
Complete tear of deep capsule ligament and partial tear of superficial
layer of MCL
○
No gross instability; slight laxity
○
Slight swelling
○
Moderate to severe joint tightness with decreased ROM
○
Pain along medial aspect of knee
○
-
Signs of injury- Grade III
Complete tear of supporting ligaments
○
Complete loss of medial stability, meniscus disruption
○
Minimum to moderate swelling
○
Immediate pain followed by ache
○
Loss of motion due to effusion and hamstring
○
-
Care
RICE for at least 24 hours
○
Crutches if necessary
○
Knee immobilizer may be applied
○
Move from isometrics and STLR exercises to bicycle riding and isokinetic
○
Return to play when all areas have returned to normal
Continued bracing may be required
§
○
-
Lateral collateral ligament sprain
Cause of injury
Result of a Varus force, generally with the fibula internally rotated
○
Direct blow is rare
○
-
Sign of injury
Pain and tenderness over LCL
○
Swelling and effusion around the LCL
○
Joint laxity with Varus testing
○
-
Care
Following management of MCL collateral ligament sprain
○
-
Anterior Cruciate Ligament Sprain
Cause: fairly common
MOI: athlete decelerates with foot planted and turns in the direction of
the planted foot forcing tibia into internal rotation
○
May be linked to inability to decelerate valgus and rotational stresses-
landing strategies
○
Male versus female injury rates
More common in female
Due to hormonal, anatomy, conditioning?□
biomechanics most likely □
§
○
Impact of femoral notch, ACL size and laxity, malalignment (Q-angle)
faulty biomechanics
○
Extrinsic factors may include, conditioning, skill acquisition, playing style,
equipment, preparation time
○
Also involve damage to other structures including meniscus, capsule, MCL
○
-
Sign
Experience pop with severe pain and disability
○
Positive anterior drawer and Lachman's
○
Rapid swelling at the joint line
○
-
Care
RICE, use of crutches
○
Arthroscopy may be necessary to determine extent of injury
○
Could lead to major instability in incidence of high performance
○
Without surgery joint degeneration may result
○
Age and activity may factor into surgical option
○
** can take a long time to heal**
○
Surgery may involve joint reconstruction with grafts (tendon)
transplantation of external structures
Will require brief hospital stay and 3-5 weeks of a race
§
Also requires 4-6 months of rehab
§
○
-
Lachman's Test
Most commonly used test for integrity of ACL
-
At 30 degrees of flexion attempt is made to translate the tibia anteriorly on the
femur
-
When it ACL is inflamed, it may show a smaller rotation
-
Posterior Cruciate Ligament Sprain
Cause of injury
Most at risk during 90 degree of flexion
○
Fail on bent knee is most common mechanism
○
Can also be damaged as a result of a rotational force
○
-
Sign
Feel a pop in the back of the knee
○
Tenderness and swelling in the popliteal fossa
○
Laxity with posterior sag test
○
-
Care
RICE
○
Non-operative rehab of grade I and II injuries should focus quad strength
○
Surgical versus non-operative care
○
-
PCL test- Posterior Drawer test
Meniscus Injuries
Cause
Medial meniscus is more commonly injured due to ligamentous
attachments and decreased mobility
Also more prone to disruption through torsional and valgus force
§
○
Result from weight bearing combined with rotation
○
-
Sign
Diagnosis is difficult
○
Effusion developing over 48-72 hour period
○
Joint line pain and loss of motion
○
Intermittent locking and giving way
○
Pain with squatting
○
-
CARE
Immediate care= PRICE
○
If the knee isn't locked, but indications of a tear are present further
diagnostic testing may be required
Treatment should follow that of MCL injury
§
○
If locking occurs, anesthesia may be necessary to unlock the joint with
possible arthroscopic surgery follow- up
○
-
Apley's compression test
Used to detect meniscus tear
-
Knee at 90 degree apply hard downward pressure with rotation
-
Pain indicates meniscal injury
-
Medial tear- external rotation
-
Lateral tear- internal rotation
-
Joint contusions (bruises)
Cause of injury
Blow to the muscles crossing the joint (varstus medial - quadriceps)
○
-
Sign
Present as knee sprain, severe pain, loss of movement and signs of acute
inflammation
○
Swelling
○
-
Knee plica
Plica: a thickened fold of synovial membrane lining the inside of the joint
capsule. 3 of them around the knee joint infra, supra, mediopatellar plica)
-
Cause
Mechanism of injury
Twisting knee with foot fixed sitting for long period of time
§
○
-
Bursitis
Cause
Acute, chronic or recurrent swelling
○
Prepatellar= contused kneeing
○
Infrapatellar= overuse of patellar tendon
○
-
Sign
Prepatellar bursitis may be localized swelling above knee that is similar to
a balloon
○
Presents with signs of inflammation (swelling, redness)
○
Swelling in back of the knee may indicate
○
-
Loose bodies (joint mice)
Cause
Result of repeated trauma
○
Possibly stems from fragments of bone or meniscal fragments, synovial
tissue or cruciate ligaments
○
-
Sign
May become lodged, causing locking or popping
○
Pain and sensation of instability
○
-
Care
If not surgically removed, it can lead to conditions causing joint
degeneration
○
-
Iliotibial band friction syndrome
"runner's knee"
-
Cause
Repetitive/ overuse conditions attributed to mal-alignment and structural
asymmetries
○
Result of repeated knee flexion and extension
○
-
Sign
Irritation at band's insertion (lateral side of the knee)
○
pain with activity
○
-
Care
Avoidance of aggravating activities
○
Correction of mal-alignments
○
Ice before and after activity, proper warm-up and stretching
○
-
Fracture of patella
Cause
Direct or indirect trauma (severe pull of tendon)
○
Forcible contraction, falling, jumping or running
○
-
Sign
Hemorrhaging with generalized swelling
○
Little bone separation with direct injury (fragments)
○
Indirect fractures may cause joint capsular tearing, separation of bone
fragments and possible quadricep tendon tearing
○
-
Management
X-ray is needed because it's a bone injury
○
Refer and immobilize for 2-3 months
○
-
-
Lecture 9
Wednesday, April 25, 2018 9:03 AM
Document Summary
Used to reveal laxity ( ) of the mcl and lcl. Valgus force moves lateral to medial (test mcl) Varus force moves medial to lateral (test lcl) A condition in which the knees angle in and can touch one another when legs are straightened. Major ligaments of the knee can be torn in isolation or in combination. Injury can result from direct line force, rotary force or combination of the two. Result of severe blow or outward twist- valgus force. Some joint stiffness and point tenderness on lateral aspect. Complete tear of deep capsule ligament and partial tear of superficial layer of mcl. Moderate to severe joint tightness with decreased rom. Loss of motion due to effusion and hamstring. Move from isometrics and stlr exercises to bicycle riding and isokinetic. Return to play when all areas have returned to normal. Result of a varus force, generally with the fibula internally rotated.