MEDI7301 Study Guide - Final Guide: Interpersonal Psychotherapy, Parathyroid Gland, Somnolence


Bipolar disorders
Bipolar disorder/ bipolar affective disorder (BPAD)
Classification
Etiology Bipolar Genetics
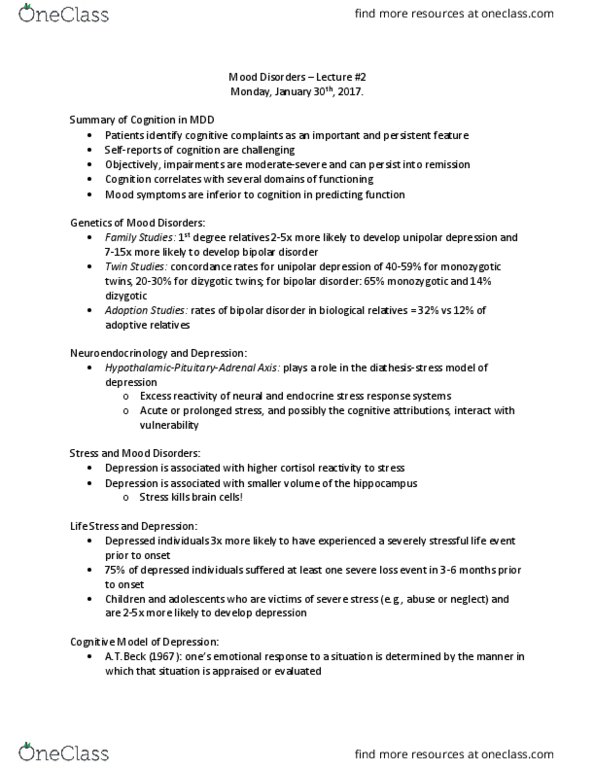
60-65% bipolar patients have family hx of major mood
disorders
First degree relatives are 7x more likely to develop bipolar
than general population
Polygenetic disease - 18q and 22q chromosome are two
regions with strongest evidence to bipolar
Neuroimaging
Reduced activation & reduced grey matter in areas
associated with emotional regulation
Increased activation in ventral limbic brain regions that
mediate and generate emotional responses
Neurotransmitters
Catecholamine hypothesis - increase in Ad and NAd causes
mania
DA & 5-HT - certain drugs (cocaine, L-dopa, amphetamines,
anti-depressants) cause mania
Environment
High SES
Stressful life events, especially pregnancy
Secondary
mania/
hypomania
Substances of abuse - amphetamine, cocaine, alcohol, opiates,
hallucinogens
Prescribed medication - corticosteroid, antidepressants, levodopa,
methylphenidate, baclofen, bromocriptine, dapsone, isoniazid, metoclopramide
General medical conditions - frontotemporal dementia, temporal
lobe epilepsy, stroke, white matter ischaemia disease (Binswanger), multiple
sclerosis, Huntington's disease, neurosyphillis, HSV encephalitis, HIV/ AIDS, SLE,
hyperthyroidism, hypothyroidism
Epidemiology &
course
M=F affected; manic more common in males & depressive more common in
females
Females are more likely to experience more depressive or mixed episodes,
rapid cycling or bipolar II
Mean age of onset - 18yrs old (bipolar 1), 20yo (bipolar 2)
Risk factors - family hx of mood disorders, upper SES class, childhood trauma, single
or separated,
Episode is defined by a change in polarity (eg mania -> baseline or mania ->
find more resources at oneclass.com
find more resources at oneclass.com

depression)
Most patients experience both depressive and manic episodes; 10-20% experience
only manic episodes
Between episodes (intermorbid functioning), bipolar patients are generally well
functioning (eg can maintain job)
Bipolar affective disorders (I, II) have an extremely variable course
It usually begins in late adolescence with subthreshold depressive sx
First episode is usually major depression (54%), mania (22%), mixed (24%)
Average 1 episode every 2yrs; mean number of episodes is 9; patients can
range from 2-30 episodes per liftime
Rapid cycling = 4 or more episodes in 12mths
Possible period of many years (eg 5+yrs) without further episode, however
length of time between subsequent episodes with begin to narrow, although most will
ultimately reach stability
Untreated patients may have 10+ episodes in lifetime, and the duration
and period of time between episodes will stabilize after 4th ot 5th episode
Kindling - recurrent mood episodes may cause gradually accumulating damage,
resulting in episodes progressing from reactive (stress triggered) to spontaneous, increasing in
frequency, becoming more severe & ultimately resistant to treatment
Prognosis (bipolar I)
Poorer prognosis than MDD patients
7% have no recurrent sx, 45% have more than 1 episode, 40% have chronic
disorder
Long term follow - 15% well, 45% well with multiple relapses, 30% partial
remission, 10% chronically ill
Risk/ predictive
factors
Episode criteria Mania/
hypomania
episode
Abnormally and persistently elevated, expansive or irritable mood
+ abnormally and persistently increased goal-directed activity or energy = mood
disturbance
oHypomania lasts 4 consecutive days; absence of psychotic
symptoms; less disruption to work/ social/ interpersonal life
oMania lasts at least 1 week (up to 4 months) or any
duration (if hospitalisation required); presence of psychosis (delusions,
hallucinations)
At least 3 of following symptoms are present during mood
disturbance (or 4 symptoms is mood is irritable)
oDistractibility - inability to censor immaterial external
stimuli (eg interviewer's attire, background noise, room furniture) and
find more resources at oneclass.com
find more resources at oneclass.com

prevents rational conversation/ following instruction
oIndiscretion - excess spending, sexual overactivity,
dangerous driving, increased sociability
oGrandiosity & inflated self esteem - uncritical self-
confidence (eg best at sport, smartest person in room), marked grandiose
delusions (eg special relationship with famous person), embark on
complex tasks (eg write a novel, initiate an impractical invention)
oFlight of ideas or racing thoughts - accelerated speech with
abrupt shifts from one topic to another
oPsychomotor agitation or increase in goal-directed activity
(eg possible catatonia/ manic stupor)
oSleep need decreases - little sleep, feel full of energy and
rested, it may last up to days of no sleep
oTalkativeness - uninterruptible, rapid, pressured speech
This episode is not attributable to substance or another medical
condition
Mania = mood disturbance is sufficient enough to cause marked
impairment in social or occupational functioning or necessitate hospitalization
to prevent harm to self or others or psychotic features present
Hypomania = mood disturbance is not severe enough to cause
marked impairment in social or occupational functioning or necessitate
hospitalization; no psychotic features present
oSymptoms are lesser degree/ severity compared to mania
Major
depressive
episode
See MDD above for criteria
Bipolar depression is more rapid in onset, more frequent, more
severe, greater amount of delusions & has atypical features/ reverse
neurovegetative sx (hypersomnia, hyperphagia, agitated)
Mixed
episode
Manic and major depressive episode criteria are both met
(excluding duration) almost every day for at least 1 week
Manic/ hypomanic episode + mixed features are episodes
that meet full criteria for mania/ hypomania + at least 3 of the following
sx during most days of the episode
oDepressed mood
oAnhedonia
oPsychomotor retardation
oLow energy
oExcessive guilt/ feelings of worthlessness
oSuicidal thoughts, behaviour or attempt
Major depressive episode + mixed features are episodes
that meet full criteria for major depression + at least 3 of the following
sx during most days of the episode
oElevated or expansive mood
oInflated self-esteem of grandiosity
oTalkativeness or pressured speech
oFlight of ideas or racing thoughts
oIncreased energy or goal-directed activity
oIndiscretion (excessive involvement in
pleasurable activities that have high potential for painful
consequences)
oDecreased sleep
Symptoms cause social/ occupational distress, hospitalization or
impairment
Symptoms are not caused by substance or medical condition
Psychosis Main features
Mood congruent sx
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
60-65% bipolar patients have family hx of major mood. First degree relatives are 7x more likely to develop bipolar than general population. Polygenetic disease - 18q and 22q chromosome are two regions with strongest evidence to bipolar. Reduced activation & reduced grey matter in areas associated with emotional regulation. Increased activation in ventral limbic brain regions that mediate and generate emotional responses. Catecholamine hypothesis - increase in ad and nad causes. Da & 5-ht - certain drugs (cocaine, l-dopa, amphetamines, anti-depressants) cause mania. Substances of abuse - amphetamine, cocaine, alcohol, opiates, hallucinogens. Prescribed medication - corticosteroid, antidepressants, levodopa, methylphenidate, baclofen, bromocriptine, dapsone, isoniazid, metoclopramide. General medical conditions - frontotemporal dementia, temporal lobe epilepsy, stroke, white matter ischaemia disease (binswanger), multiple sclerosis, huntington"s disease, neurosyphillis, hsv encephalitis, hiv/ aids, sle, hyperthyroidism, hypothyroidism. M=f affected; manic more common in males & depressive more common in. Females are more likely to experience more depressive or mixed episodes, rapid cycling or bipolar ii.