MEDI7302 Study Guide - Final Guide: Cirrhosis, Cholecystectomy, Insulinoma


Pancreas
Learning
objectives
Describe the interpretation of serum lipase levels to diagnose pancreatitis and
formulate a differential diagnosis for the causes of pancreatitis
Contrast acute mild with acute severe pancreatitis and explain the management
options
Outline the features of chronic pancreatitis
Describe the typical symptoms for and the approach to investigation of a patient
with a lesion in the pancreatic head
Acute
pancreatitis
Acute inflammation of pancreas involving auto-digestion of pancreas via premature
activation of pancreatic enzymes inside pancreas
Normal physiology
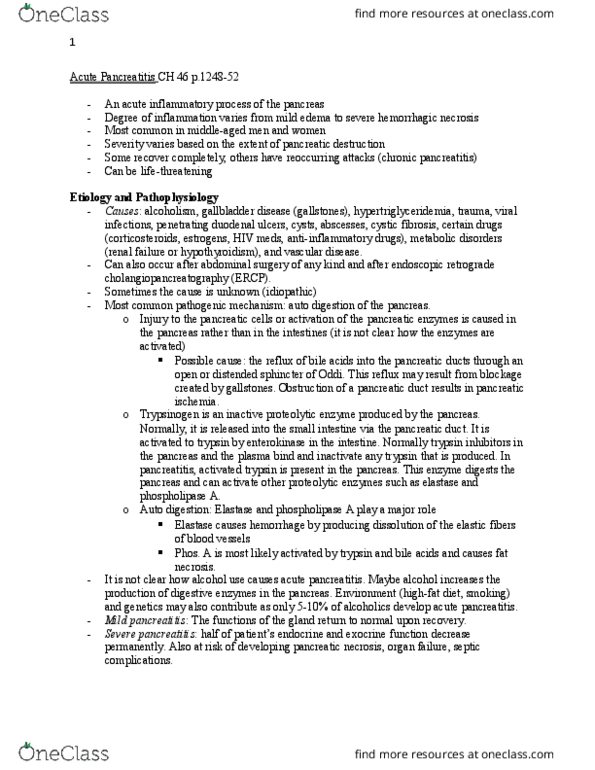
Pancreas has endocrine function (insulin production via a-cells and b-cells)
and exocrine function (manufacture and secrete digestive enzymes for carb, fat and
protein metabolism)
80% gross weight supports exocrine function VS 20% is involved with
endocrine function
Exocrine synthesis
oInactive digestive enzymes are produced by acinar cells as
zymogens (pre-cursor to active enzyme), packed in storage vesicles with protease
inhibitors (collectively called zymogen granules) and released via pancreatic duct
cells into pancreatic duct
oZymogen granules have acidic pH and low Ca concentration to
protect against premature activation until secretion occurs
oFood ingestion and CCK signalling stimulates release of zymogens
into pancreatic duct and duodenum -> pancreatic trypsinogen (pancreatic zymogen)
is activated into trypsin once it encounters brush border enzyme enterokinase at
duodenum -> trypsin activates pancreatic proenzymes
o-ve feedback mechanism stimulated (elevated trypsin -> decreased
CCK and secretin -> limit pancreatic secretion)
Pathogenesis
80% cases are mild-moderate; severe cases may have intra-pancreatic
bleeding, serious tissue damage, infection and fluid collection; possible damage to other
organs including lungs and kidneys
Inciting event -> acinar cell injury OR impaired release of zymogens ->
lysosomal and zymogen granules fuse to enable trypsinogen to trypsin activation ->
intracellular trypsin triggers intra-pancreatic activation of digestive enzymes (amylase,
lipase) -> autodigestion and inflammation (TNFa, IL6) -> increased pancreatic vascular
permeability (hemorrhage, oedema, pancreatic necrosis)
oFirstly, acute oedematous pancreatitis - parenchymal oedema and
peripancreatic fat necrosis (via lipase activation)
oNext, liquefactive hemorrhagic necrosis (liquefied pancreas,
parenchymal necrosis, hemorrhage and dysfunction of gland)
find more resources at oneclass.com
find more resources at oneclass.com

oPossible pseudocyst (enzymes walled off by granulation tissue) or
pancreatic abscesses (bacterial seeding of pancreatic or peripancreatic tissue)
Mediators may leak into systemic circulation, causing bacteremia (gut flora
translocation), ARDS, pleural effusions, GI hemorrhage, renal failure, SIRS and shock
Etiology (I GET SMASHED)
Idiopathic Occult microlithiasis
Gallstones 40% cases, leading cause of acute pancreatitis
Transient or persistent obstruction of AoV via
gallstones or sludge -> increasing pancreatic duct pressure -> acinar cell
injury
Ethanol 35% cases
Alcohol increases zymogen release from acinar cells
-> alcohol decreases fluid and HCO3 in ducts, causing thickened
pancreatic juices that can plug/ block pancreatic duct -> increased
backwards pressure and duct distension
oAt cellular level, membrane trafficking
becomes chaotic -> zymogen granules may fuse with lysosomes ->
premature activation of trypsinogen to trypsin, hence activating
zymogens
Alcohol stimulates cytokine release via acinar cells
-> immune response (neutrophils release superoxide and proteases)
Alcohol oxidative metabolism produces ROS ->
damage pancreatic cells
Trauma Blunt trauma
Seatbelt injury in acceleration-deceleration +/- triple
A, L1 chance fracture, mesenteric hemorrhage)
Bike handlebar injury in kids (handlebar hits right in
epigastrium), giving red dot sign
Surgery Post-ERCP - 1% risk (severe pancreatitis) or 10% risk
(mild pancreatitis)
Malignancy/
microbiological
Head of pancreas carcinoma (painless jaundice)
Mumps, CMV, coxsackie
Autoimmune SLE, PAN, Crohn, CF
Sting Trinidad (scorpion), Aus (funnel web, brown snake)
Hyper-Ca, hyper-
TG
TG > 1000mg/dL
Hyper-TG is best identified in recurrent pancreatitis
(acute phase usually has elevated TG since fat necrosis is common)
Emboli/
ischaemia
Global ischaemia from sepsis, burns
Drugs Steroids
Thiazide diuretics
Signs and sx
Sudden onset of dull epigastric pain radiating to back, aggravated by
eating, relieved with sitting forward
Possible nausea, vomiting, anorexia, sweating
Fever, tachycardia, hypotension, abdominal tenderness, guarding, rebound
tenderness, distension/ ileus
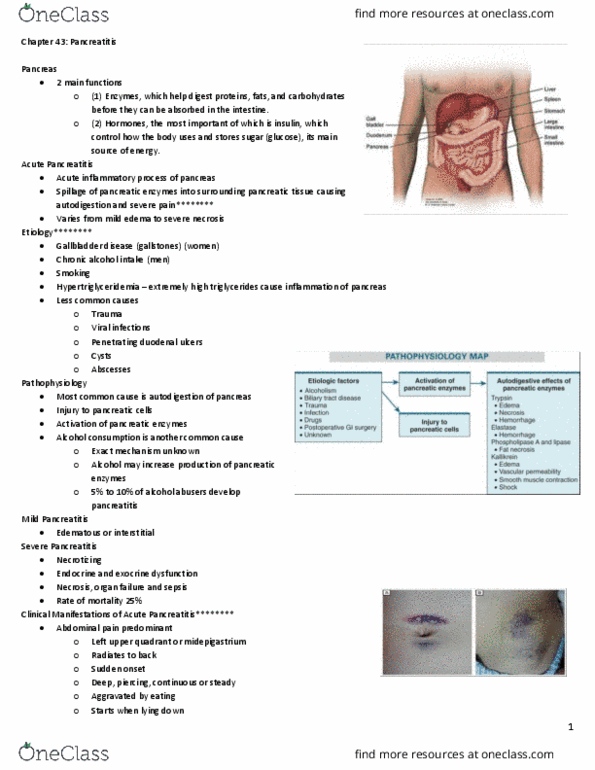
Severe necrotizing pancreatitis
oCullen sign - bluish discolouration around umbilicus from
hemoperitoneum (remnant of umbilical artery tracks to portal hepatis in falciform
ligament)
oGrey-Turner sign - reddish-brown discolouration along flanks
from retroperitoneal blood
oErythematous skin nodules from focal subcut fat necrosis
Investigations
Diagnostic pancreatic lipase (most specific, typically increases 3-6hrs after
onset + peak within 24hrs + remain elevated for 8-14 days, 3x normal amount)
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Describe the interpretation of serum lipase levels to diagnose pancreatitis and formulate a differential diagnosis for the causes of pancreatitis. Contrast acute mild with acute severe pancreatitis and explain the management options. Describe the typical symptoms for and the approach to investigation of a patient with a lesion in the pancreatic head. Acute inflammation of pancreas involving auto-digestion of pancreas via premature activation of pancreatic enzymes inside pancreas. Pancreas has endocrine function (insulin production via a-cells and b-cells) and exocrine function (manufacture and secrete digestive enzymes for carb, fat and protein metabolism) 80% gross weight supports exocrine function vs 20% is involved with endocrine function. Inactive digestive enzymes are produced by acinar cells as zymogens (pre-cursor to active enzyme), packed in storage vesicles with protease inhibitors (collectively called zymogen granules) and released via pancreatic duct cells into pancreatic duct o. Zymogen granules have acidic ph and low ca concentration to protect against premature activation until secretion occurs o.