MEDI7302 Study Guide - Final Guide: Pap Test, Chemokine, Enterococcus


UTIs and Renal Calculi
Learning
objectives
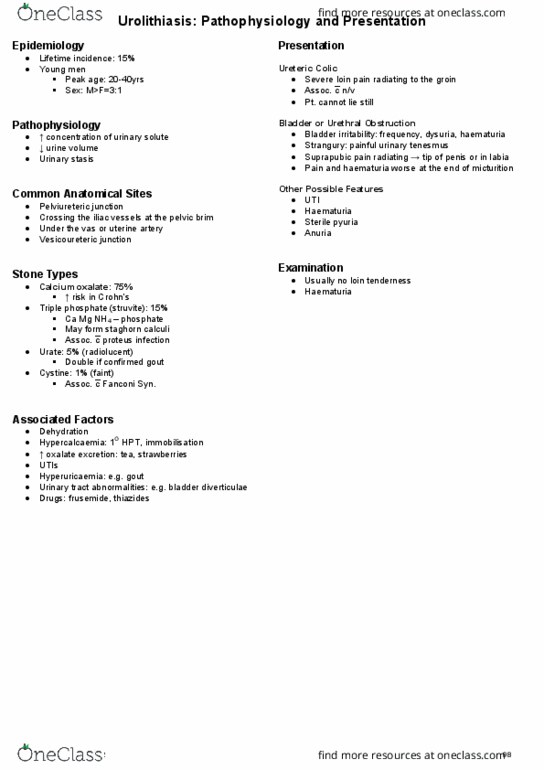
Outline the factors contributing to urinary tract calculi formation
Describe how urinary tract calculi can present
Discuss the medical and surgical approaches to management of renal tract calculi
List the risk factors for urinary tract infection
Outline the pathophysiology, presentation and management of obstructive
urosepsis
Renal + ureteric
calculi
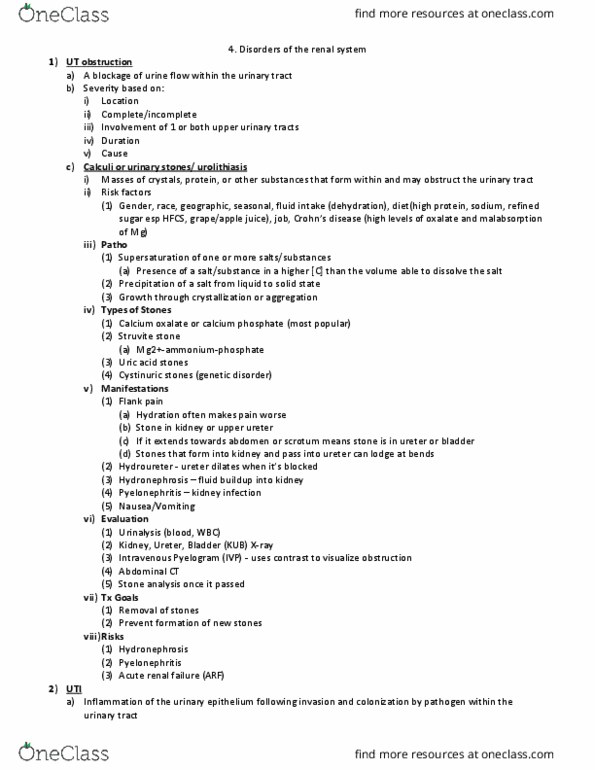
Stone types Common Calcium oxalate (most common 70%)
Black/ dark brown stone, radio-opaque
XR, form in acidic urine
Uric acid (2nd most common)
Red/ brown stone, radio-lucent XR
(transparent, not visible)
Breakdown product of purines
Calcium phosphate
Dirty white stone, radio-opaque XR, form
in alkaline urine
Magnesium ammonium phosphate (struvite)
Infection stone
Mg + NH3 + PO4
Dirty white, radio-opaque XR
Bacteria (proteus mirabilis, proteus
vulgaris, morganella morganii) breakdown urea into
CO2/NH3 via urease -> NH3 makes urine more alkaline,
increasing precipitation of NH3 Mg PO4 into staghorn
calculi (branch into several renal calyces)
Rare Cystine (AA)
Yellow or light pink stone, radio-opaque
XR
Xanthine (byproduct of purine breakdown)
Red-brown stone, radiolucent XR
Drug metabolites
Matrix
Pathogenesis Little genetic basis
High concentration of urine solutes causing supersaturation ->
solutes precipitate out and crystalize into stones -> act as nidus for further
crystallisation
Increase in solutes
Decrease in solvent (dehydration status (low fluids))
Geographical - warmer climates/ seasons
Environmental - dietary factors (Ca supplements), dehydration
Genetic - hyper-oxaluria, cystine stones, storage diseases
Risk factors (via stone type)
Ca stones - hyper-calcaemia (increased GIT absorption,
hormonal causes eg hyper PTH), hyper-calciuria (impaired renal
tubular rebsorption)
Ca oxalate stones - hyper-oxaluria (Ca oxalate stones
only) via genetic defect (increase oxalate excretion), liver metabolism
defect OR diet heavy in oxalate-rich foods (eg rhubarb, spinach,
chocolate, nuts, beer)
Uric acid stone - high purine consumption (eg shellfish,
anchovies, red meat)
Struvite stone - UTIs, vesico-ureteral reflux, obstructive
uropathy
Diagnosis History + exam
find more resources at oneclass.com
find more resources at oneclass.com

Imaging - XR, CT scan, US
Urinalysis - microscopic or gross hematuria
History Possible presentations
Pain
Dull or localised flank pain (mid-lower back) + renal colic
pain (misnomer; sharp constant pain) both caused by distension,
stretching and spasm of ureteric wall around obstructing stone
Colicky or constant (nature), severe (intensity), loin-to-
groin (location), usually hrs of pain (duration), sudden and rapid
(onset/offset), possible radiation to testis or labia majora
Associated features - nausea, sweating, shaking,
vomiting
Alleviated by movement, nil aggravation factors
Haematuria
Usually microscopic hematuria
Macroscopic hematuria - old blood with 'tea staining' or
coca-cola coloured urine (not fresh blood), usually with renal colic at
time or preceded by pain, large upper tract stones or anti-coagulant
patients
Painless hematuria is caused by a urothelial carcinoma
unless proven otherwise
Recurrent UTIs
Stones may be a source of recurrent UTIs caused by
same organism
Staghorn calculus - high index of suspicion for proteus
UTI
Sepsis
Sepsis is a life threatening condition not to be missed
(hypotensive, tachycardiac, peripherally shut down patient may have
renal obstruction 2* to stone)
Suspect in diabetic, immunocompromised or elderly
patients
Irritative voiding
Final passage of stone through intramural ureter
(traversing layers of bladder detrusor) may give painless irritative
voiding
Increased frequency and urgency, small volume voids,
constant desire to void & incompleteness post-void
Discomfort post-void
Painless passage of stone or incidental finding on imaging
(abdominal US)
Anuria in patients with solitary kidney
Other relevant
hx
Hx findings increasing risk of stone presence
Previous stones/ stone rx, fam hx stones
Hx gout, bowel disease
Chemotherapy, bowel surgery, stoma
O/E Observe movements with or without pain (peritonitis is not
indicative of stone)
Ill or well looking, vital signs
Renal angle punch
External genitalia + DRE/VE
Investigations Mid stream urine
FBC, U&E
Non-contrast CT scan - rule out AAA leak
Plain XR
Management Rapid diagnosis and exclusion of other pathology (esp life-
threatening)
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Outline the factors contributing to urinary tract calculi formation. Discuss the medical and surgical approaches to management of renal tract calculi. List the risk factors for urinary tract infection. Outline the pathophysiology, presentation and management of obstructive urosepsis. Red/ brown stone, radio-lucent xr (transparent, not visible) Dirty white stone, radio-opaque xr, form in alkaline urine. Bacteria (proteus mirabilis, proteus vulgaris, morganella morganii) breakdown urea into. Co2/nh3 via urease -> nh3 makes urine more alkaline, increasing precipitation of nh3 mg po4 into staghorn calculi (branch into several renal calyces) High concentration of urine solutes causing supersaturation -> solutes precipitate out and crystalize into stones -> act as nidus for further crystallisation. Ca stones - hyper-calcaemia (increased git absorption, hormonal causes eg hyper pth), hyper-calciuria (impaired renal tubular rebsorption) Ca oxalate stones - hyper-oxaluria (ca oxalate stones only) via genetic defect (increase oxalate excretion), liver metabolism defect or diet heavy in oxalate-rich foods (eg rhubarb, spinach, chocolate, nuts, beer)