NURS 303 Study Guide - Final Guide: Latent Autoimmune Diabetes Of Adults, Impaired Glucose Tolerance, Diabetes Mellitus Type 2


Diabetes:
- Type 2 diabetes increases the risk of coronary heart disease more markedly in women than men.
- DM more affecting women, the older adult, the obese and the less educated.
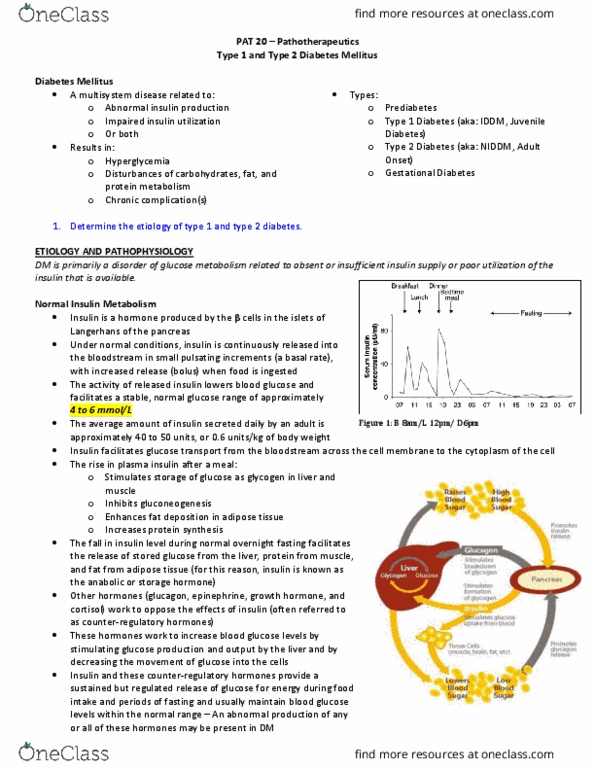
Normal Insulin Metabolism:
- insulin is a hormone produced by the B cells in the islets of Langerhands of the pancreas
- normal glucose 4-6 mmol
- avg. amount of insulin secreted 40-50 units or 0.6 units/kg of body weight
- counter regulatory hormones: glucagon, epinephrine, growth hormone→ work to increase blood
glucose levels by stimulating glucose production and output by the liver and by decreasing the movement
of glucose into the cells.
- Insulin is released from the pancreatic B cells as a precursor, proinsulin and is then routed through the
liver
- Insulin facilitates glucose transport from the bloodstream across the cell membrane to the cytoplasm of
the cell
- Rise in insulin after meal stimulates storage of glucose as glycogen liver and muscle, inhibits
gluconeogenesis, enhances fat deposition in adipose tissue and increases protein synthesis.
- the fall in insulin during overnight fasting facilitates the release of stored glucose from the liver, protein
from the muscle and fat from adipose tissue-→ Why insulin is called the anabolic or storage hormone.
Type 1 Diabetes Mellitus:
- younger than 30, 11-13 yrs
- typically seen with people with lean body type
- latent autoimmune diabetes in adults (LADA)= describe the small number of people with apparent type
2 DM who appear to have immune-mediated loss of pancreatic B cells.
- results from destruction of pancreatic B cells owing to an autoimmune process
- related to human leukocyte antigens
- HLA types associated with an increased risk for type 1 DM include HLA-DR3 and HLA-DR4
- long pre-clinical period
- islet- cell antibodies responsible for B cell destruction are present for months to years before onset of
symptoms
- patient usually has a history of recent and sudden weight loss as well as the classic symptoms of
polydipsia, polyuria, polyphagia
- Honeymoon period: the patient requires very little injected insulin because B cell mass remains
sufficient for glucose control as the progressive destruction continues to occur→ lasts 3-12 months
Prediabetes:
- impaired glucose tolerance or impaired fasting glucose
- noted when a fasting or 2-hour plasma glucose level is higher than normal
- usually no symptoms
- 6.1-6.9 mmol of IFG, or 7.1-11 mmol/L for IGT
Type 2 Diabetes Mellitus:
- usually in people other than 35 yrs
- 80-90% overweight
- risks: obesity or abdominal weight . Visceral adipocytes release an excess amount of free fatty acids
which are associated with insulin resistance at the level of the liver as well as several adipocytes.
find more resources at oneclass.com
find more resources at oneclass.com

- membership in high risk population: aboriginal, Hispanic, south Asian
- Acanthosis Nigricans is a cutaneous sign of an underlying condition and is characterized by a velvety,
light brown to black hyperpigmented thickening of the skin, usually on the back the side of the neck and
the axillae.
- three times higher in people with schizophrenia
- pancrease usually continues to produce some endogenous insulin.
- four major metabolic abnormalities have a role in the development of type 2 DM
1) insulin resistance in glucose and lipid metabolism which is a condition in which body tissues
do not respond to the action of insulin. Insulin recetors that are unresponsive to the action of insulin,
insufficient in number or both. Most receptors are located on skeletal muscle, fat and liver cells.
- insulin mediates glucose uptake into fat tissue and skeletal muscle through GLUT4 glucose transporters.
- insulin resistance is associated with a decreased in the number of GLUT4 transporters—resultsin
hyperglycemia
2) type 2 DM is a marked decrease in the ability of the pancreas to produce insulin.
3) inappropriate glucose production by the liver→ instead of properly regulating the release of
glucose in response to blood levels, the liver does so in haphazard way that does not correspond to the
body’s needs at the time. There is an increased secretion of glucagon from the alpha cells of the pancrease
that stimulates glucose production by the liver, adding to the increase in blood sugar.
4) fourth factor is alteration in the production of hormones and cytokines by adipose tissue=
adipocytokines which appear to play a role in glucose and fat metabolism.
- 2 main ones adiponectin and leptin
Metabolic syndrome: cluster of abnormalities that act synergistically to greatly increase the risk for
cardiovascular disease. Characterized by abdominal obesity, hypertension, dyslipidemia, insulin
resistance, dysglycemia.
- abdominal obesity, sedentary lifestyle, urbanization and westernization and certain ethnicities
Gestational Diabetes:
- between 24 and 28 weeks of gestation
- treatment reduced perinatal death and neonatal complications such as birth trauma, hypoglycemia,
hyperbilirubinemia and respiratory distress syndrome.
- physical activity should be encouraged
- risk of developing type 2 DM is greater post
Secondary Diabetes:
- occurs because of another medical condition or as a result of treatment of medical condition that causes
abnormal blood glucose levels.
- may be caused by schizophrenia, cystic fibrosis, cushing’s syndrome, hyperthyroidism,
immunosuppressive therapy, corticosteroids, phenytoin, atypical antipsychotics.
Clinical Manifestations of Type 1 DM:
- polyuria, polydipsia, polyphasia
- polyphasia= consequence of cellular malnourishment when insulin deficiency prevents utilization of
glucose for energy.
- weight loss may occur because of the body cannot get glucose and turns to other energy sources such as
fat and protein.
find more resources at oneclass.com
find more resources at oneclass.com

- pronounced changed in visual acuity owing to changes in the lens with hyperglycemia and fluid
retention. Women may have vaginal yeast infections.
Type 2 DM clinical Manifestations:
- fatigue, recurrent infections, prolonged wound healing, visual acuity changes, painful peripheral
neuropathy of the feet.
Complications:
- diagnosis of type 1 DM 4 things:
- hemoglobin A1C > 6.5%
- fasting glucose level of > 7 mmol/L (fasting is defined as no caloric intake for at least 8 hours)
- random or casual plasma glucose > 11.1/L
- 2 hour OGTT Level > 11.1 mmol
- A1C is good indicator because fasting is not required and there are fewer day-to-day alterations during
periods of stress and illness.
- glycosylated hemoglobin
- amount of glucose that has been attached to hemoglobin molecules which are attached to the red
blood cell for the life of the cell (120 days)
- ideal for people with DM is 7% or less
- target of A1C of less than 6.5% can be considered in some patients with type 2 DM to further
lower the risk of neuropathy
Collaborative Care:
- goal: promote well-being, reduce symptoms, prevent acute complications of hyperglycemia and
hypoglycemia and delay the onset and progression of long term complications
Types of Insulin:
- human biosynthetic insulin is now the most widely used insulin
- Basal-bolus regimen: uses rapid or short acting (bolus) insulin before meals and intermediate or long
acting (basal).
- Intensive Insulin Therapy= basal-bolus therapy= multiple daily insulin→ goal is to achieve a near-
normal glucose of 4-7 mmol/L before meals
Meal Time Insulin (Bolus)
- rapid-acting
- lispro Humalog
- apart insulin, novorapid
- glulisine, apidra
- when rapid actin insulin is used as mealtime coverage in people with type 1 DM, additional and longer
acting insulin must also be used as basal background inslulin because the duration of rapid actin insulin is
so short
Long or Intermediate-Acting (basal) background insulin:
- glargine (lantus)
- detemir (Levemir)
- extended long acting basal insulins that are released steadily and continuously over 24 hours
- they lack oeak action time so the risk for hypoglycemia is greatly reduced
- clear colourless insulins
- glargine and detemir must not be diluted or mixed with any other insulin or solution
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Type 2 diabetes increases the risk of coronary heart disease more markedly in women than men. Dm more affecting women, the older adult, the obese and the less educated. Insulin is a hormone produced by the b cells in the islets of langerhands of the pancreas. Avg. amount of insulin secreted 40-50 units or 0. 6 units/kg of body weight. Counter regulatory hormones: glucagon, epinephrine, growth hormone work to increase blood glucose levels by stimulating glucose production and output by the liver and by decreasing the movement of glucose into the cells. Insulin is released from the pancreatic b cells as a precursor, proinsulin and is then routed through the liver. Insulin facilitates glucose transport from the bloodstream across the cell membrane to the cytoplasm of the cell. Rise in insulin after meal stimulates storage of glucose as glycogen liver and muscle, inhibits gluconeogenesis, enhances fat deposition in adipose tissue and increases protein synthesis.