Pharmacology 2060A/B Study Guide - Midterm Guide: Phases Of Clinical Research, Thiopurine Methyltransferase, Adrenergic Receptor

27 Dec 2013
School
Department
Course
Professor

Document Summary
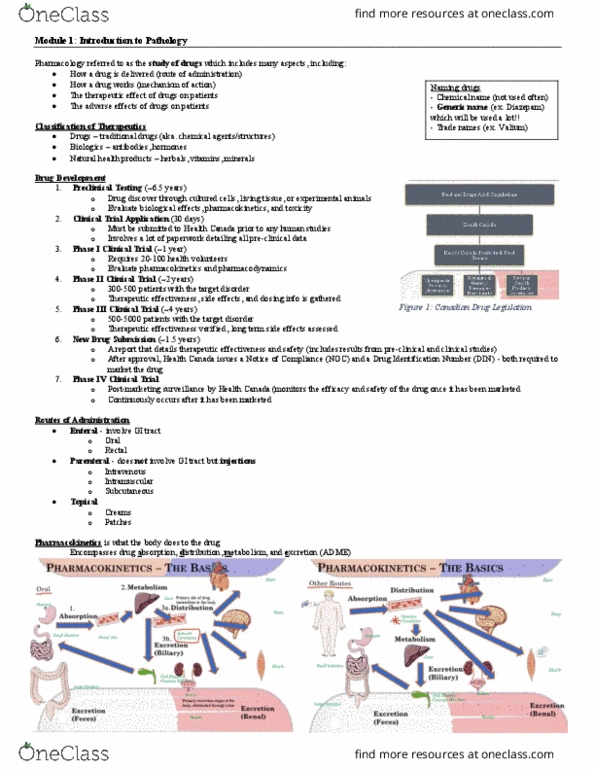
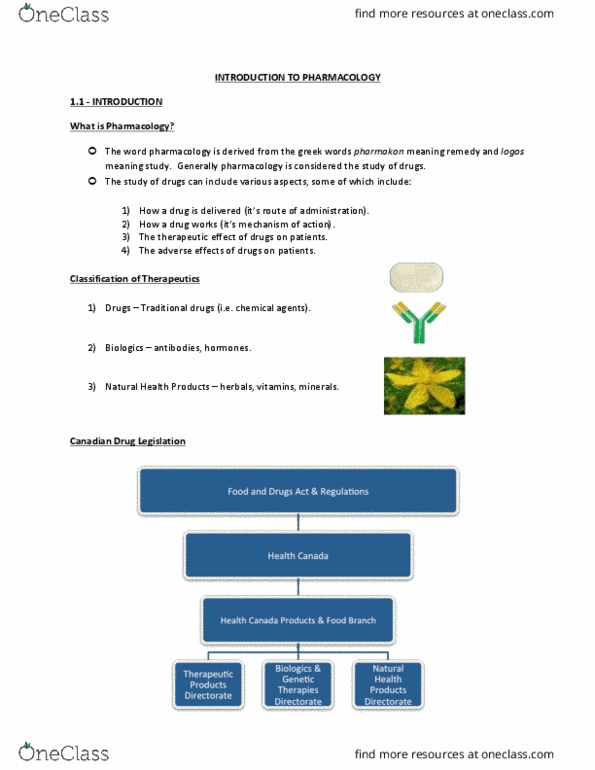
Clinical trial application: submitted to health canada prior to human studies. New drug submission (nds) submitted to health canada; details therapeutic effectiveness & safety. If approved, health canada issues a notice of compliance (noc) and a drug information. Phase iv clinical trial: post marketing surveillance; monitor efficacy and safety of drug. Oral drug tissues stomach small intestine portal vein liver (metabolism) systemic circulation gall bladder via bile duct . Parenteral injection; absorbed from injection site into systemic circulation, bypasses liver. fecal excretion (secondary) large intestine . Ions mostly, not every small ion can pass through a channel, depends on charge. Uptake transporters: intestinal absorption, renal excretion and reaching target action site inside cell. Efflux transporters: intestine, placenta, kidney and at bbb. Alpha 1 acid glycoprotein: for hydrophilic basic drug. Cyp: (12) families of drug metabolizing phase 1 enzymes, oxidize drugs. Liver, kidney diseases, inflammation and infection decrease cyp activity.