NURS 2550H Chapter Notes - Chapter 49: Renal Vein, Hypotension, Gluconeogenesis

28 Jun 2018
School
Department
Course
Professor

Chapter 49: Acute Kidney Injury
Definitions:
- Renal Replacement Therapy (RRT): all forms of life-supporting therapies for renal
therapies for renal failure including hemodialysis, peritoneal dialysis, hemofiltration, and
renal transplantation.
- Acute Kidney Injury (AKI): renal impairment that ranges from mild, calling for little
intervention, to severe, necessitating renal replacement therapy; the changes in renal
function are acute in nature and usually occur over a 48-hour period.
- Acute Renal Failure (ARF): The advanced stages of acute kidney injury that call for
aggressive management and often necessitate renal replacement therapy.
- Prerenal causes of AKI: those that reduce renal blood flow and lead to decreased
glomerular perfusion and filtration
- Intrarenal causes of AKI: conditions that cause direct damage to the renal tissue, resulting
in impaired nephron function.
- Postrenal causes of AKI: mechanical obstruction of urinary outflow. As the flow of urine
is obstructed, urine refluxes into the renal pelvis, impairing kidney function.
- Acute Tubular Necrosis (ATN): necrosis of the renal tubular cells caused by nephrotoxic
substances or ischemia.
- Hemodialysis: A type of dialysis that uses a machine to remove waste products and
excess fluid from the blood by pumping the blood through an artificial semipermeable
membrane
- Oliguria: a urine output of less than 400 mL in 24 hours
- Uremia: a constellation of signs and symptoms resulting from the buildup of waste
products and excess fluid associated with kidney failure; they may include elevated
serum creatinine and blood urea nitrogen, abnormal electrolytes, acidosis, anaemia, fluid
volume excess, nausea, loss of appetite, fatigue, decreased cognition, pruritus, and
neuropathy
Intro to Kidney Disease:
- Kidney disease can result in the inability to excrete metabolic waste products and water
as well as functional disturbances of all body systems.
- Acute kidney injury (AKI) has a rapid onset.
- Chronic kidney disease (CKD) usually develops slowly over months to years. If CKD
progresses to stage 5 renal replacement therapy (RRT) (dialysis or transplant) is
necessary for long-term survival.
- CKD is much more common in the older population
Acute Kidney Injury:
- also, known as acute renal failure (ARF)
- an abrupt decline in kidney function leading to a rise in serum creatinine or a reduction in
urine output, or both.
- Potentially can be reversed but the mortality rate is high
- AKI usually affects people with life-threatening conditions.
- Severe AKI develops in over 60% of critical care unit patients, with mortality rates of 70
to 80%
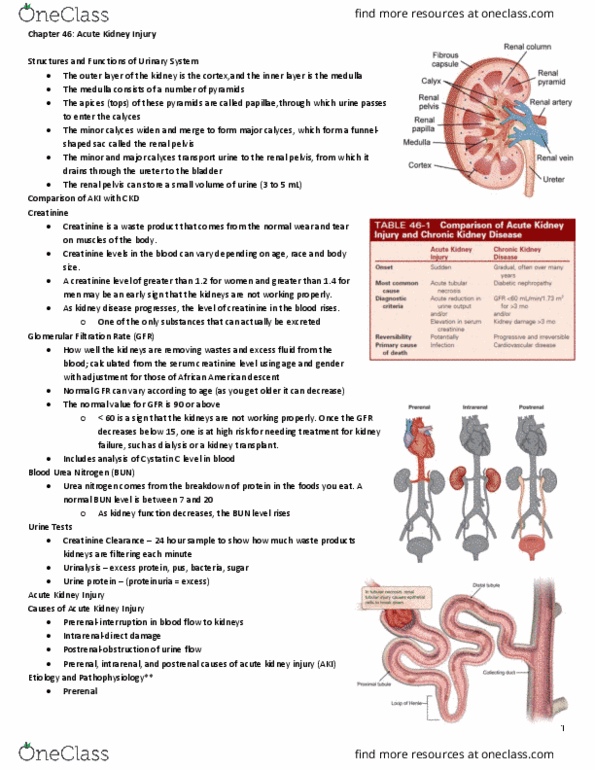
Etiology and Pathophysiology:
- Causes leading to AKI with renal failure are divided into prerenal, intrarenal (intrinsic)
and postrenal
find more resources at oneclass.com
find more resources at oneclass.com

- Prerenal causes of AKI are those that reduce renal blood flow and lead to decreased
glomerular perfusion and filtration
- With a decrease in circulating blood volume, autoregulatory mechanisms that increase
angiotensin II, aldosterone, norepinephrine, and antidiuretic hormone attempt to preserve
blood flow to essential organs. Prerenal azotemia (high levels of nitrogen containing
products in the blood) results in a reduction in the excretion of sodium, increased salt and
water retention, and decreased urine output.
- Prerenal AKI can also be caused by vasoactive medication such ACE inhibitors, that
cause intrarenal vasoconstriction leading to hypoperfusion of the glomeruli.
- Usually reversible, may develop into intrarenal if not treated promptly
- Intrarenal causes include conditions that cause direct damage to the renal tissue
(parenchyma), resulting in impaired nephron function.
- Intrarenal causes of AKI are usually owing to prolonged ischemia or the presence of
nephrotoxins, hemoglobin released from hemolyzed RBCs, or myoglobin released from
necrotic muscle cells
- Nephrotoxins can cause obstruction of intrarenal structures by crystallization or by
actually damaging the epithelial cells of the tubules.
- Hemoglobin and myoglobin can block the tubules and cause renal vasoconstriction
- Acute tubular necrosis (ATN) is the most common intrarenal cause of AKI and is primary
the result of ischemia, nephrotoxins, or sepsis.
Severe renal ischemia causes a disruption in the basement membrane and diffuse
destruction of the tubular epithelium
Nephrotoxic agents cause necrosis of tubular epithelial cell, which slough off and
plug the renal tubules
- Possible pathological processes involved in ATN include the following:
1. Hypovolemia and decreased renal blood flow stimulate renin release, which
activates the renin-angiotensin-aldosterone system and results in constriction of
the peripheral arteries and the renal afferent arterioles. With decreased renal
blood flow, there is decreased glomerular capillary pressure and GFR as well as
tubular dysfunction and oliguria.
2. Ischemia alters glomerular epithelial cells and decreases glomerular capillary
permeability. This reduces the GFR, which significantly reduces blood flow and
leads to tubular dysfunction.
3. When tubules are damaged, interstitial edema occurs, and necrotic epithelia cells
accumulate in the tubules. The debris lowers the GFR by obstructing the tubules
and increasing intratubular pressure.
4. Glomerular filtrate leaks back into plasma through holes in the damaged tubular
membranes, which decreases intratubular fluid flow.
- Postrenal causes of AKI involve mechanical obstruction of urinary outflow. As the flow
of urine is obstructed, urine refluxes into the renal pelvis, impairing kidney function.
- Postrenal AKI is treatable if found early
Common Causes of AKI
Prerenal Intrarenal
Hypovolemia Prolonged prerenal ischemia
Dehydration Nephrotoxic injury
Hemorrhage Drugs (aminoglycoside, amphotericin B)
find more resources at oneclass.com
find more resources at oneclass.com

GI losses (diarrhea, vomiting) Radiocontrast agents
Excessive diuresis Hemolytic blood transfusion reaction
Hypoalbuminemia Severe crush injury
Burns Chemical exposure (ethylene, glycol,
lead, arsenic, carbon tetrachloride)
Decreased CO Acute glomerulonephritis
Cardiac dysrhythmias Thrombotic disorders
Cardiogenic shock Toxemia of pregnancy
HF Malignant HTN
MI Systemic lupus erythematosus
Pericardial tamponade Interstitial nephritis
Pulmonary edema Allergies (antibiotics, NSAIDs, ACE
inhibitors)
Valvular heart disease Infections (bacterial, viral, fungal)
Decreased peripheral vascular resistance Postrenal
Anaphylaxis Benign prostatic hyperplasia
Antihypertensive drugs Cancer (bladder, prostate, cervical,
colorectal)
Neurological injury Calculi formation
Septic shock Neuromuscular disorders
Decreased renovascular blood flow Spinal cord disease
Bilateral renal vein thrombus Strictures
Embolism Trauma (back, pelvis, perineum)
Hepatorenal syndrome
Renal artery thrombosis
Clinical Manifestations:
- Can be corrected by correcting the cause
- If parenchymal damage has occurred from either prerenal or postrenal causes, or
intrarenal causes, ATN results and the course of AKI is prolonged. ATN progresses
through 3 stages:
- Initiation Phase: Increase in serum creatinine and BUN and a decrease in urine output.
- Maintenance Phase: During this phase patients may be anuric, oliguric, or nonoliguric. A
dilute urine is made but uremic toxins are not being removed. The nurse must be alert for
sings and symptoms of these changes.
- Urinary Changes:
omost common initial manifestation of ATN is oliguria, which is when urine
output generally decreases to less than 400 mL/24h.
oIf ATN is caused by ischemia, oliguria will occur within 24 hours
oIf ATN is caused by nephrotoxic drugs, the onset may be delayed for as long as a
week.
oUrine sediment may show RBCs and WBCs, casts, and proteinuria.
- Fluid Volume Excess:
oWhen urinary output decreases, fluid retention occurs.
oThe severity of the symptoms depends on the extent of the fluid overload.
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Renal replacement therapy (rrt): all forms of life-supporting therapies for renal therapies for renal failure including hemodialysis, peritoneal dialysis, hemofiltration, and renal transplantation. Acute kidney injury (aki): renal impairment that ranges from mild, calling for little intervention, to severe, necessitating renal replacement therapy; the changes in renal function are acute in nature and usually occur over a 48-hour period. Acute renal failure (arf): the advanced stages of acute kidney injury that call for aggressive management and often necessitate renal replacement therapy. Prerenal causes of aki: those that reduce renal blood flow and lead to decreased glomerular perfusion and filtration. Intrarenal causes of aki: conditions that cause direct damage to the renal tissue, resulting in impaired nephron function. Postrenal causes of aki: mechanical obstruction of urinary outflow. Acute tubular necrosis (atn): necrosis of the renal tubular cells caused by nephrotoxic substances or ischemia.