PHTY208 Lecture Notes - Lecture 15: Chest Injury, Kyphosis, Pancreatic Duct


Disorders of ventilation
• Learning Outcomes
o For the following respiratory disorders, describe the:
• pathology
• aetiology
• pathogenesis
• effects on chest wall compliance, lung compliance, airway resistance and respirato
ry mechanics (pathophysiology)
• effects on O2, CO2 and secretion movement (pathophysiology)
• clinical manifestations
o Infective disorders
• Acute bronchitis
• Pneumonia
o Obstructive disorders
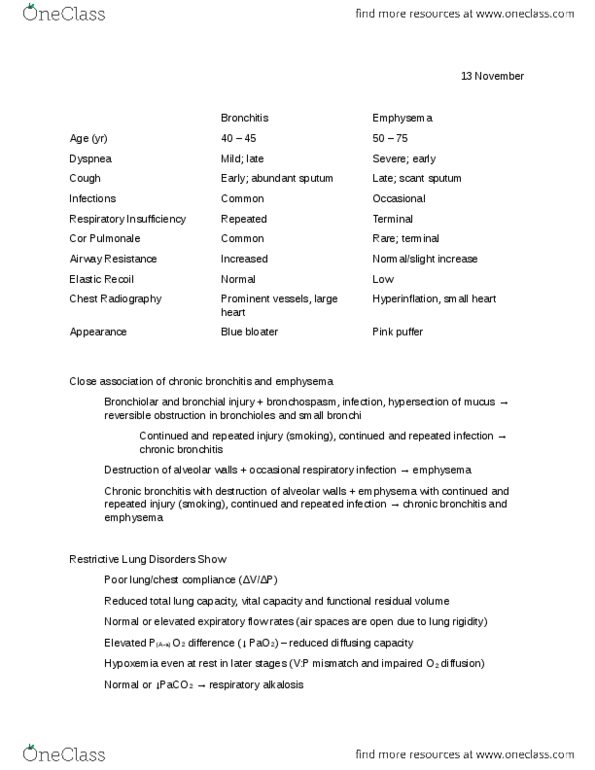
• Chronic bronchitis
• Emphysema
• Asthma
o Restrictive disorders
• Interstitial lung disease
• Chest wall disorders
o Suppurative disorders
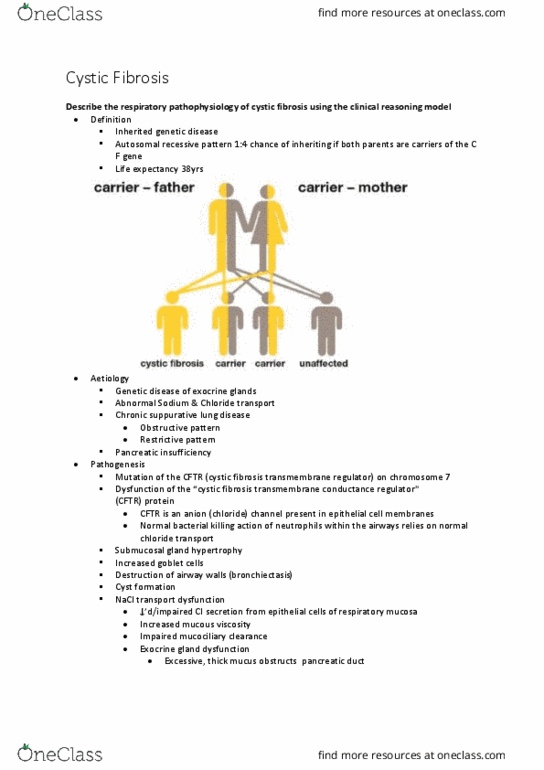
• Cystic fibrosis
• No‐CF bronchiectasis
o Disorders of the pleural space
• Pneumothorax
• Haemothorax
• Pleural effusion
o Disorders of the pulmonary circulation
• Right heart failure
• Cor pulmonale
• Revision of terminology
o Pathology
• The interruption, cessation, disorder or disease of a body system or organ
structure
o Aetiology
• the cause, set of causes, or manner of causation of a disease or condition
o Pathogenesis
• The sequence of cellular and tissue events that take place from the time of
initial contact with an aetiological agent until the ultimate expression of the
disease i.e. how the disease process evolves
o Pathophysiology
• The study of the ods response to dysfunction or disease.
o Clinical manifestations
• Symptoms
▪ Patient reported subjective outcomes
• Signs
▪ Objective outcomes measured by observations, examination, tests, scales
• Airways defence mechanisms
o Normal airways defence mechanisms
find more resources at oneclass.com
find more resources at oneclass.com

• Lungs are usually sterile
• Upper airway is colonised by benign anaerobic bacteria which limit invasion
by more pathogenic bacteria
o 3 major risks to the respiratory system
• Inspired air
• Pulmonary circulation
• Flooding of the alveoli
o Mechanical and Anatomical defences
• Nasal passages
▪ Filter & humidify air
• Upper airway reflexes
▪ Epiglottis & bulbar muscles minimise aspiration
• Mucociliary escalator
▪ Mucous glycoprotein produced by goblet cells, trap particles
▪ Traps & clears foreign particles
• Cough
▪ Clear mucous & particles from lower airways
• Lymphatics
▪ Drain fluid from interstitium & assist immune response
o Cellular Lung Defences
• Alveolar macrophages reside in alveoli and survey alveolus for foreign material
which they internalise, phagocytose and inactivate
• They also release chemical mediators to recruit neutrophils.
• Neutrophils increase phagocytic activity due to large numbers that are rapidly recr
uited
• Natural killer lymphocytes target virally infected and other o‐
self cells for apoptosis by releasing membrane permeabilising enzymes.
o Molecular Lung Defences
• Include cytokines, prostaglandin E2, cell wall hydrolases, iron binding proteins, co
mplement components, defensins, anti-proteinases, surfactant proteins and
antioxidants
• Surfactant – protects alveoli from collapse according to Laplace's Law P=4T/r
• Infective Disorders
o Upper respiratory tract infection (URTI)
• Definition
▪ Infection of the respiratory system involving anatomical structures including
the larynx and above e.g. the common cold
• Aetiology
▪ Usually viral (±bacterial)
• Pathogenesis
▪ Immune and inflammatory response
• Clinical manifestations
▪ Increased mucus production
▪ Constitutional symptoms (see acute bronchitis)
o Acute bronchitis
• Definition
▪ Reversible bronchial inflammation and mucus production
• Aetiology
▪ Infection of the lower respiratory tract in 95% of cases viral in origin
(influenza)
▪ Fifth most common condition diagnosed by Australian GPs
find more resources at oneclass.com
find more resources at oneclass.com

• Pathogenesis
▪ An infectious or non infectious trigger leads to bronchial epithelial injury,
which causes an inflammatory response with airway hyper responsiveness
and mucus production.
• Clinical manifestations
▪ Signs and symptoms
• Cough illness lasting less than 2 to 3 weeks
• ±Sputum
• Dyspnoea
• Frequently accompanied by other upper respiratory tract and
constitutional symptoms
• Headache, fever, myalgia, malaise, sore throat, rhinorrhoea
▪ Auscultation
• ±Wheeze
• ±Crackles
o Pneumonia
• Definition
▪ Inflammation of the lung parenchyma due to the presence of a micro-
organism
▪ May be acute or chronic
• Aetiology
▪ Bacteria, fungal or viral
▪ Aspiration of pathogens from oropharyngeal or nasopharyngeal flora (most
common)
▪ Inhalation of other irritating substances e.g. gastric contents
▪ Inhalation of iro‐orgaiss e.g. legionella
▪ Bacteria are spread into the lungs in the blood from bacteraemia e.g.
infected IV site
▪ Direct inoculation or spread e.g. tracheal intubation, stabbing
▪ Infection only occurs when organisms overcome the normally effective
lung defence mechanisms - as a result of either lungs' defences being
defective or overwhelmed by the virulence or quantity of organisms
• Risk factors
▪ Age
▪ Immunocompromised individuals
▪ Chronic respiratory disease
▪ Alcoholism
▪ Altered level of consciousness
▪ Smoking
▪ Malnutrition
▪ Immobilisation
• Acute pneumonia
▪ Usually bacterial
▪ Induces primarily neutrophilic exudate in alveoli, bronchioles and bronchi
• Chronic pneumonia
▪ Usually fungi, parasites and intracellular bacteria
▪ Chronic inflammatory response
• Pathology: common microorganisms
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Learning outcomes: for the following respiratory disorders, describe the, pathology aetiology, pathogenesis, effects on chest wall compliance, lung compliance, airway resistance and respirato ry mechanics (pathophysiology, effects on o2, co2 and secretion movement (pathophysiology) clinical manifestations. Infective disorders: acute bronchitis, pneumonia, obstructive disorders, chronic bronchitis, emphysema, asthma, restrictive disorders. Signs: objective outcomes measured by observations, examination, tests, scales, airways defence mechanisms, normal airways defence mechanisms. Lungs are usually sterile: upper airway is colonised by benign anaerobic bacteria which limit invasion by more pathogenic bacteria, 3 major risks to the respiratory system. Flooding of the alveoli: mechanical and anatomical defences, nasal passages. Filter & humidify air: upper airway reflexes, epiglottis & bulbar muscles minimise aspiration, mucociliary escalator, mucous glycoprotein produced by goblet cells, trap particles, traps & clears foreign particles, cough, clear mucous & particles from lower airways. Include cytokines, prostaglandin e2, cell wall hydrolases, iron binding proteins, co mplement components, defensins, anti-proteinases, surfactant proteins and antioxidants.