PHYS 799 Lecture Notes - Lecture 15: Multiple Endocrine Neoplasia, Nissl Body, Nipple Discharge

23 Apr 2019
Department
Course
Professor
Document Summary
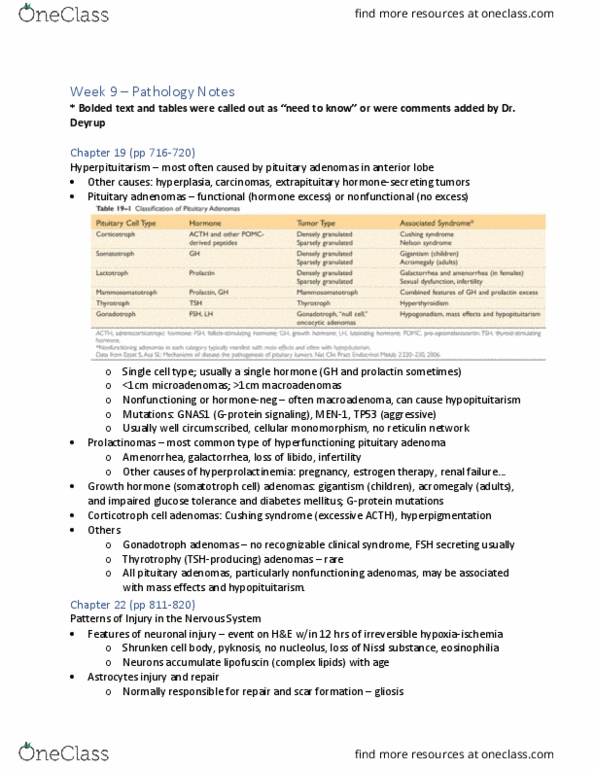
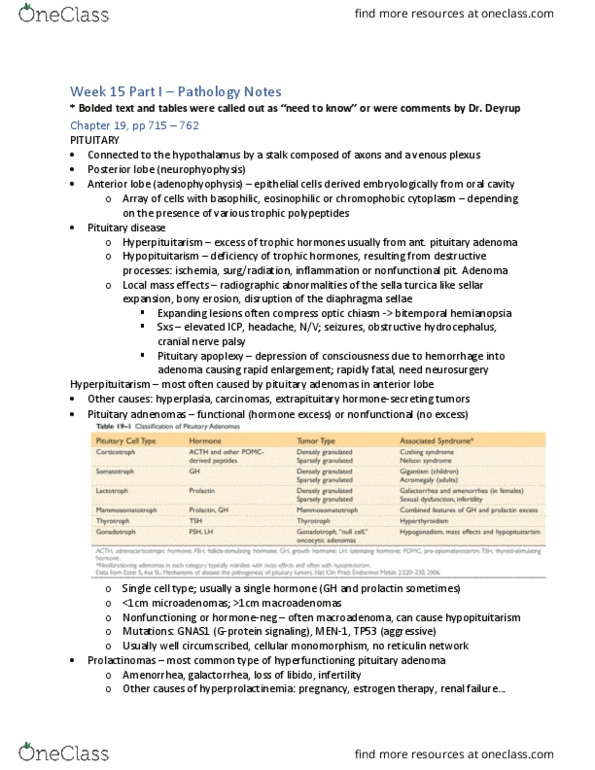
Nonfunctioning adenomas may destroy adjacent parenchyma hypopituitarism. Functional = assoc. w/hormone excess, causes clinical signs; nonfunctioning = clinically silent adenoma (which produces hormone) or hormone-negative adenoma. Mutation in alpha subunit of gs constitutive activation is common in gh-secreting adenomas; tp53 mutations assoc. w/aggressive behavior (atypical adenoma) Inherited adenomas: men1 (multiple endocrine neoplasia syndrome i), cdkn1b, prkar1a, aip. Morphology: well-circumscribed, soft lesion; uniform (monomorphic) polygonal cells, w/limited mitotic activity; sparse ct (reticulin); cytoplasm can be acidophilic, basophilic, chromophobic. 30% are nonencapsulated; can invade bone, dura, brain. Prolactinoma most common; causes amenorrhea, galactorrhea (milky nipple discharge), loss of libido, infertility; effects less obvious in men and older women. Gh-producing (somatotroph cell) adenoma 2nd most common; often small amts of prolactin also; causes hepatic secretion of igf1 gigantism (large body, long arms/legs) in children; acromegaly (prominent jaw, large hands/feet, enlarged organs) Gh can also cause dm, muscle weakness, hypertension, arthritis, osteoporosis, chf.