MEDI7302 Study Guide - Final Guide: Ethology, Hernia Repair, Chronic Obstructive Pulmonary Disease


Hernia
Learning
objectives
Explain the anatomy of the abdominal wall including the inguinal and femoral canals
Contrast the presentation of epigastric, umbilical, inguinal, femoral and Spigelian
hernias
Outline the causative factors for and presentation of incisional hernias
Describe the difference between reducible and irreducible hernias and the
implications for bowel within a hernia
Formulate a differential diagnosis for a lump in the groin
Definition +
epidemiology
Hernia is an abnormal protrusion of a viscus/ part of viscus through a defect, either
in the containing wall of that viscus OR within the cavity the viscus is situated in
Epidemiology
Hernia prevalence & risk of strangulation increases with age
5% general population develops an abdominal wall hernia -> 75% inguinal
hernias
M:F ratio is 25:1
Indirect inguinal hernias are more common than direct inguinal hernias
Femoral hernias are more common in F > M
External hernias
Abnormal protrusion of intra-abdominal tissue through fascial defect in
abdominal wall
Inguinal (80%), incisional (10%), femoral (5%), umbilical (4%), epigastric,
other
Internal hernias
Intestine passes beneath constricting band or through peritoneal window
within abdominal cavity or diaphragm
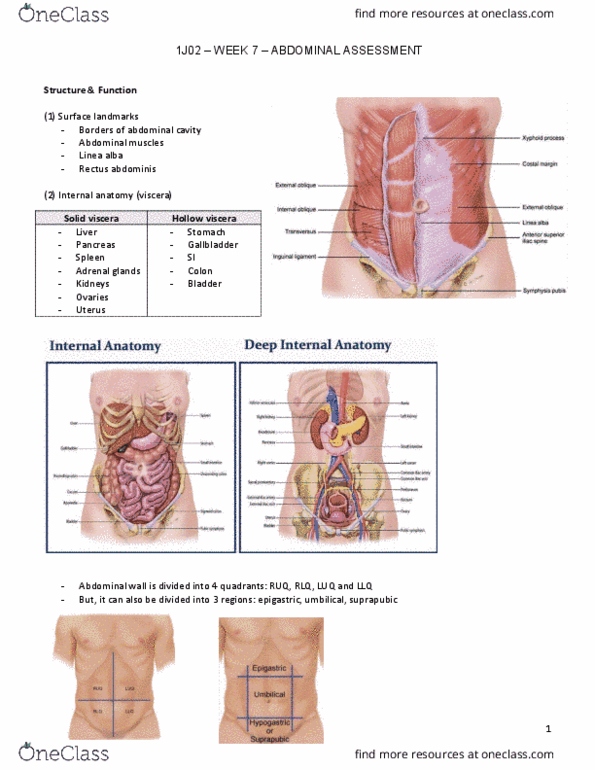
Anatomy Anterior abdominal wall
Wall layers Skin
Subcutaneous tissue
Fascia
Campers (fatty superficial)
Scarpas (fibrous deep)
Muscle
External oblique (forms inguinal ligament in groin)
Internal oblique
Rectus abdominis
Transverse abdominis
Fascia transversalis
Peritoneum
Midline +
rectus
sheath
EOM, IOM and TM aponeuroses all insert into linea alba
Arcuate line is located about 1/3 distance from pubic crest
find more resources at oneclass.com
find more resources at oneclass.com

to umbilicus (3-6cm below umbilicus)
Demarcation line of internal oblique and
transversus aponeurosis of rectus sheath passing anteriorly to rectus
abdominis muscle, leaving transversalis fascia posteriorly
Above arcuate line
Anterior layer of rectus sheath (in front of rectus
abdominis) = external oblique aponeurosis + half of internal oblique
aponeurosis
Posterior layer of rectus sheath (behind rectus
abdominis) = half of internal oblique aponeurosis + transversus muscle
aponeurosis + transversalis fascia
Below arcuate line
Anterior layer of rectus sheath = external oblique
aponeurosis + internal oblique aponeurosis + transversus muscle
aponeurosis
No posterior layer of rectus sheath, only
transversalis fascia
Inferior epigastric arteries enter rectus sheath at arcuate
line
Inguinal canal
Description 4cm long canal extending inferiorly-medially from
internal (deep) inguinal ring -> external (superficial) inguinal ring; it lies
superior and parallel to inguinal ligament
Deep internal ring - midpoint of inguinal
ligament, lateral to epigastric vessels, created by transversalis fascia
Superficial external ring - superior to pubic
tubercle, created by evagination of external oblique
Boundaries (MALT)
Roof - transversus abdominus muscle, internal
oblique muscle
Anterior wall - external oblique aponeurosis,
internal oblique aponeurosis
Floor - inguinal ligament, lacunar ligament
Posterior wall - conjoint tendon (common
aponeurotic insertion of IOM and TM), transversalis fascia
Gender differences
Males - inguinal canal contains spermatic cord
oTesticular artery, cremasteric artery, vas
deferens artery
oGenitofemoral nerve, cremasteric nerve
(branch off genitofemoral), SNS fibres
oPampiniform plexus, ductus deferens,
lymphatics (to para aortic nodes)
oNOTE: ilioinguinal runs alongside cord
Females - inguinal canal contains round ligament
Important landmarks
Mid-inguinal point - midpoint of pubic symphysis
and ASIS; femoral pulse
Midpoint of inguinal ligament - midpoint of pubic
tubercle and ASIS (2 attachments of inguinal ligament); deep inguinal
ring opening to inguinal canal above this point
Hesselbach's triangle (boundaries of inguinal canal floor)
Inferior epigastric vessels (superolateral)
Rectus sheath (medial)
Inguinal ligament (inferior)
find more resources at oneclass.com
find more resources at oneclass.com

Diagram
Femoral canal
Description An anatomical compartment 1.3cm long within the
femoral triangle that is the smallest, most medial part of the femoral sheath
Boundaries
Medial - lacunar ligament
Lateral - femoral vein
Anterior - inguinal ligament
Posterior - pectineal ligament (Cooper's
ligament)
Contents
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Explain the anatomy of the abdominal wall including the inguinal and femoral canals. Contrast the presentation of epigastric, umbilical, inguinal, femoral and spigelian. Outline the causative factors for and presentation of incisional hernias. Describe the difference between reducible and irreducible hernias and the implications for bowel within a hernia. Formulate a differential diagnosis for a lump in the groin. Hernia is an abnormal protrusion of a viscus/ part of viscus through a defect, either in the containing wall of that viscus or within the cavity the viscus is situated in. Hernia prevalence & risk of strangulation increases with age. 5% general population develops an abdominal wall hernia -> 75% inguinal. Indirect inguinal hernias are more common than direct inguinal hernias. Femoral hernias are more common in f > m hernias. Abnormal protrusion of intra-abdominal tissue through fascial defect in abdominal wall. Inguinal (80%), incisional (10%), femoral (5%), umbilical (4%), epigastric, other.