PHTY206 Lecture Notes - Lecture 23: Percutaneous, Avascular Necrosis, Skin Grafting


Fractures of tibia, ankle and foot
• Introduction
o It is important to remember that fractures of the lower limb below the knee often
occur in isolation and the role of the physiotherapist is to ensure safe and
independent mobility, maintenance of adjacent joints and assessment of circulatory
and respiratory status.
o It is useful to revise information on neuro-vascular checks, circulo-respiratory
exercises, lower limb maintenance exercises and education of gait with crutches in
conjunction with this module.
• Basic Physiotherapy Principles
o Healing Time
• Casts may often be removed as early as six weeks post fracture and the
patient allowed to progressively weight bear.
• This does not mean that the fracture has consolidated but that it is clinically
stable (evidence of bridging callous formation on x-ray).
• Fractures of the tibia generally heal in 12-16 weeks but can take up to 24
weeks.
o Weight Bearing
• As a general rule patients with fractures of the lower limb below the knee will
mobilise with restricted weight bearing from NWB to PWB for at least six
weeks.
• Weight bearing orders should always be confirmed in the chart or with the
surgeon.
o Crutch Walking
• Following isolated fracture patients will often be on the ward for only a very
short period of time (sometimes 1-2 days) before discharge. The role of the
physiotherapist is to teach the patient how to mobilise safely, NWB, TWB or
PWB on an appropriate aid.
• Often crutches will be the aid of choice, however occasionally it may be more
appropriate to use a hopper frame.
• When teaching crutches the following elements should be addressed:
▪ Sit to stand to sit
▪ Safe static standing
▪ Hop to/hop through gait pattern
▪ Safe turning
▪ Stairs
▪ Crutch maintenance and precautions for use (nerve palsy)
• Review PHTY 103 content on walking aids and gait e-education using those
aids
o Warnings
• Warnings for sensory and circulatory changes should be performed in the
presence of a short leg Plaster of Paris (SLPOP).
find more resources at oneclass.com
find more resources at oneclass.com

• Placing items down the cast can cause the under-wrap to bunch and result in
a pressure area, therefore it is important to warn the patient
o Neuro-vascular compromise
• Many patients with fractures distal to the knee will be managed in a short leg
POP.
• Swelling can accumulate under the cast and compromise neuro-vascular
function.
A routine check for sensation on exposed skin and capillary refill in the nail
bed at the toes should be done at initial and subsequent reviews
• Fractures of Tibial Shaft
o Mechanism of Injury
• The tibia is the most commonly fractured long bone in the body and also the
most common compound fracture due to its subcutaneous position.
• Fractures may occur due to indirect injury that is usually low energy, or due to
direct injury that is usually high energy.
• The fracture pattern will vary with the mechanism of injury such that a
twisting injury associated with sporting activities or a fall in an osteoporotic
individual may cause a spiral or oblique fracture, whilst high energy trauma
may result in a transverse or comminuted fracture.
• Fibula fractures can occur due to direct impact and in conjunction with a tibia
fracture, however they are often stable due to the stability provided by the
tiia, ad do’t euie othopaedi aageet
o Clinical Signs of tibia fracture
• Pain and deformity are noted at the location of the fracture.
• Local swelling is common and immediate neuro-vascular compromise can
occur making neurovascular assessment a priority
• Vascular status should be assessed and function of the tibial and peroneal
nerves should be monitored.
find more resources at oneclass.com
find more resources at oneclass.com

o Classifications
• Tibial shaft fractures can be classified through description with the tibia
divided into proximal, middle and distal thirds and the pattern of fracture
divided into spiral, oblique, transverse or comminuted fractures.
• The Gustilo Classification of open fractures is used to describe associated soft
tissue damage
▪ This is due to the high occurrence of open or compound fractures in this
region.
o Conservative Management
• Conservative management can be considered for isolated tibial fractures that
are either stable or undisplaced.
• Management involves immobilisation of the knee in a long leg cast, with
subsequent functional bracing and therefore knee stiffness and
quadriceps/hamstring atrophy are unavoidable.
o Surgical Management
• Required for unstable tibial shaft fractures, tibial shaft fractures in patients
with multiple injuries, fractures extending to the knee or ankle joints and tibial
shaft fractures with ipsilateral lower limb fractures.
• The options for surgical management include Open Reduction Internal
Fixation (ORIF) using intramedullary nails or plates, and External Fixation.
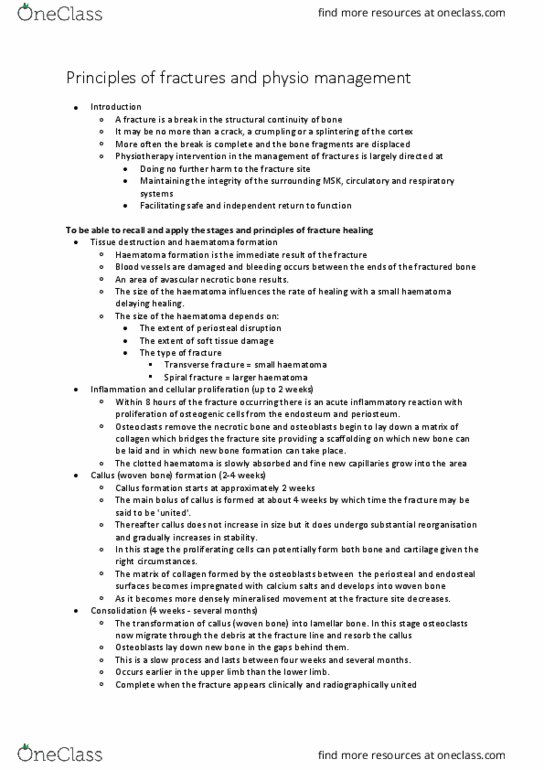
• Open Reduction Internal Fixation (ORIF)
▪ Insertion of a locked intramedullary nail is
the treatment of choice for unstable tibial
shaft fractures.
▪ The nail can be statically or dynamically
locked to provide added stability.
▪ Intramedullary nailing allows early knee
mobilisation and maintenance of
quadriceps and hamstring strength.
▪ An alternative to intramedullary nailing is
the use of plates and screws.
• This was previously the treatment of
choice however ORIF using plates and
screws has been associated with high
rates of complications such as wound
break down, infection and fracture
non-union.
• External Fixation
▪ Can be used both for temporary
(emergency) and definitive management of
tibial shaft fractures.
▪ Indicated for compound fractures, severely comminuted fractures or
tibial shaft fractures in patients with multiple trauma.
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Following isolated fracture patients will often be on the ward for only a very short period of time (sometimes 1-2 days) before discharge. The role of the physiotherapist is to teach the patient how to mobilise safely, nwb, twb or. Pwb on an appropriate aid: often crutches will be the aid of choice, however occasionally it may be more appropriate to use a hopper frame, when teaching crutches the following elements should be addressed: Swelling can accumulate under the cast and compromise neuro-vascular function. A routine check for sensation on exposed skin and capillary refill in the nail bed at the toes should be done at initial and subsequent reviews. Fractures of tibial shaft: mechanism of injury, the tibia is the most commonly fractured long bone in the body and also the most common compound fracture due to its subcutaneous position.