PHTY207 Lecture Notes - Lecture 20: Carpometacarpal Joint, Scaphoid Fracture, Metacarpal Bones

Document Summary
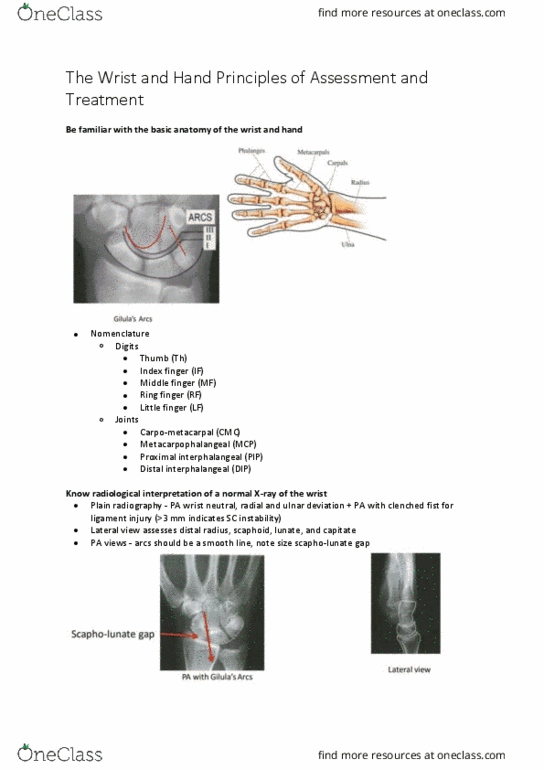
Understand which are the routine radiographic projections to evaluate pathological conditions of the hand and wrist: hand, posteroanterior, demonstrates the hand, wrist, and distal forearm. The metacarpal of the thumb is farthest from the receptor and is somewhat magnified: despite the superimposition of the wrist and forearm, displacement of a fracture fragment is easily detected on this view. Displacement is described as being in a dorsal or volar direction. Fractures of the middle and proximal phalangeal shafts may be classified as stable, unstable, or intra-articular. Fractures of the proximal phalanx angulate palmarly owing to action of the interosseous muscles, which flex the proximal fragment and extend the distal fragment. Rolando fracture, are more complicated due to joint disruption: bennett. Susceptibility due to: acts as the principal block to excessive wrist df, accepts compressive forces from the capitate and the thumb axis. Imaging: routing radiographs plus ulnar deviation, protocol is to immobilise for 10-14 days, even with no radiological evidence.