BIOL10002 Lecture Notes - Angiotensin-Converting Enzyme, Aquaporin 2, Kilogram


Week 7
Lecture 18
Respiration, part 2
Lung Structure
Trachea (cartilage in rings) Bronchi (discontinuous cartilage) Bronchiole (no cartilage) Alveoli (little sacs –
maximum surface area)
mucociliary escalator
Gills Lungs
invaginated extension of the body surface invaginated internalised extension of body surface
highly folded to increase surface area
protected by a specialised cover (operculum) protected by ribs and thorax
pumping mechanism moves water over gills ventilation mechanism moves air in & out of lungs
internal circulatory system distributes blood throughout the gill and body internal circulatory system distributes blood throughout the gill and body
have filaments which have raised folds called lamellae increase SA
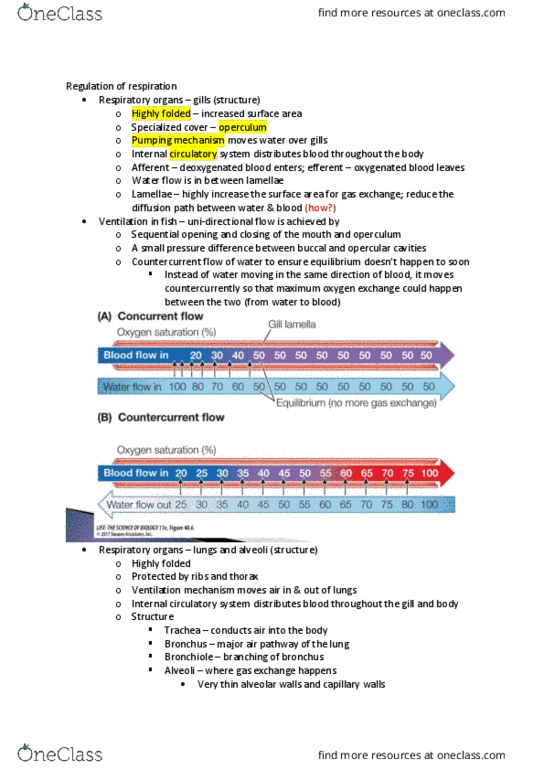
unidirectional flow of water achieved by opening and closing of the
mouth and operculum
blood flows in opposite direction to water (counter current flow)
Respiratory organs
Trachea conducts air into the body Bronchi are the major air passageway of the lung branch into bronchioles
alveoli
Exchange surface is the alveoli (epithelial cells exchange of oxygen from and into capillaries)
very thin epithelial layer – easy for pathogens to enter lungs trapped by mucous and cilia (mucous escalator goes
up trachea, and is then swallowed and killed by pH in stomach)
Lung surfactant
- A surfactant reduces the surface tension of a liquid
- lung surfactant is a phospholipoprotein secreted by some alveolar cells
- Results in less force required to inflate lungs
- Respiratory Distress Syndrome (RDS) – preterm baby – surfactant produced late in term so if baby is pre-term then
there won’t be surfactant and the baby’s lungs could collapse.
Mammalian ventilation system
- Inhalation: diaphragm naturally sits in an arc and gets pulled down
- pulls down on thoracic cavity and pleural membranes
- air enters through the trachea, and lungs expand (negative pressure)
- Exhalation: muscles all relax (diaphragm, thoracic) (positive pressure)
- Pleural membranes line the pleural cavity – if ‘punctured’ then pleural fluid fills that section of the lungs inhibiting
effective gas exchange
Regulation of ventilation and respiration
- can be both involuntary and voluntary
- sensory inputs sent to central nervous system to help brain decide depth, amplitude, frequency of breaths
Phrenic nerve – contraction and lowering of diaphragm
Efferent nerves – intercostal muscles
- Chemoreceptors on the ventral surface of the medulla = sensitive to changes in pH i.e. large increase in PO2
- Chemoreceptors in the aortic and carotid bodies are sensitive to increases in CO2 and large decreases in PO2
- Breathing rate more sensitive to increased CO2 than decreased O2, but animals in water in opposite
- build-up of CO2 causes change in pH
find more resources at oneclass.com
find more resources at oneclass.com

Hypoxia – short term effects of high altitude
Hyperventilation – big breaths in little ones out, setting new low of CO2 levels, and abnormally low CO2 level results
failure in the urge to breathe; allows free divers to go longer under water without feeling the urge to breath before
hitting the blackout zone, people can drown very easily
- anaerobic metabolic pathways
- increased BPG (2,3-bisphosphoglyceric acid) – lowers the affinity of haemoglobin for O2
long term effects of high altitude
- Reset the thresholds of the chemoreceptors for O2 so that they are more sensitive to low PO2
- Increase the number of red blood cells and blood Hb content (increases O2 capacity of the blood)
- Reduction in blood O2 stimulates production of erythropoietin in the kidney and liver. This acts on bone marrow to
produce more red blood cells
Stuff that shouldn’t happen
Cigarettes immobilise the cilia in the airways for hours increases chance of infection
smokers cough – can’t clear mucous from airways
Cystic fibrosis – mucous unusually thick and obstructs airways. Caused by a gene mutation that results in a non-
functional chloride channel, so chloride ions cannot leave the cells, which prevents the concentration gradient that
makes water leave the cell which would dilute the mucous from forming.
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Trachea (cartilage in rings) bronchi (discontinuous cartilage) bronchiole (no cartilage) alveoli (little sacs maximum surface area) Mucociliary escalator invaginated extension of the body surface invaginated internalised extension of body surface. Trachea conducts air into the body bronchi are the major air passageway of the lung branch into bronchioles alveoli. A surfactant reduces the surface tension of a liquid. Lung surfactant is a phospholipoprotein secreted by some alveolar cells. Results in less force required to inflate lungs. Respiratory distress syndrome (rds) preterm baby surfactant produced late in term so if baby is pre-term then there won"t be surfactant and the baby"s lungs could collapse. Inhalation: diaphragm naturally sits in an arc and gets pulled down. Pulls down on thoracic cavity and pleural membranes. Air enters through the trachea, and lungs expand (negative pressure) Exhalation: muscles all relax (diaphragm, thoracic) (positive pressure)