MEDI7111 Lecture Notes - Lecture 7: Bradycardia, Cardiomyopathy, Ascending Aorta


Cardiovascular 7
Pathology of the CVS
Atheroma/Atherosclerosis
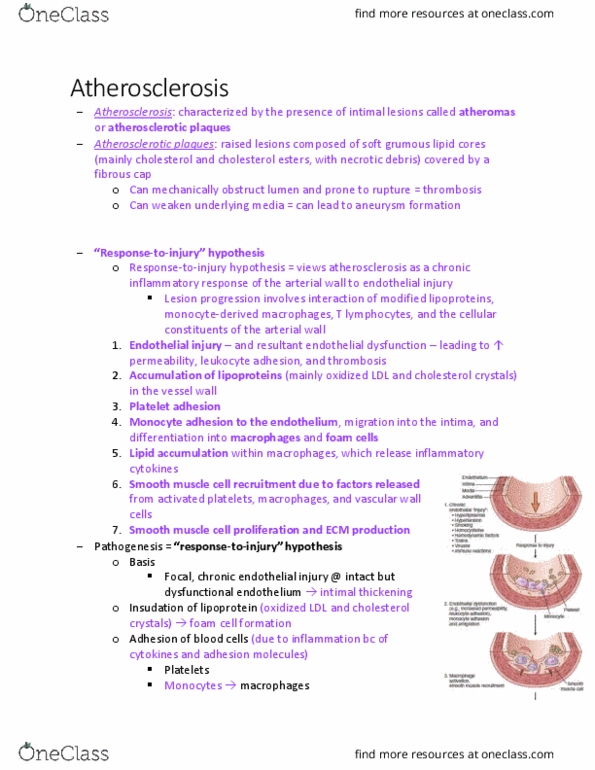
Endothelial injury and dysfunction , causing (among other things) increased vascular
permeability, leukocyte adhesion, and thrombosis
Accumulation of lipoproteins (mainly LDL and its oxidized forms) in the vessel wall
Monocyte adhesion to the endothelium , followed by migration into the intima and
transformation into macrophages and foam cells
Platelet adhesion
Factor release from activated platelets, macrophages, and vascular wall cells, inducing
smooth muscle cell recruitment, either from the media or from circulating precursors
Smooth muscle cell proliferation, extracellular matrix production , and recruitment of T
cells.
Lipid accumulation both extracellularly and within cells (macrophages and smooth
muscle cell)
find more resources at oneclass.com
find more resources at oneclass.com

Coronary Artery Disease
CAD is atherosclerosis of the coronary arteries and is the commonest cause of MI and angina.
Ischaemic Heart Disease
IHD is a group of conditions which cause ischemia to the heart; namely angina and MI.
Angina
Angina is the condition associated with ischemia to the heart which does not result in infarction.
There are three types of angina; stable, unstable and Prinzmetal.
Stable angina is chest pain that occurs on exertion and resolves on rest. Unstable angina is the
progression of stable angina whereby the chest pain occurs without correlation to activity. Both
stable and unstable anginas are due to atherosclerotic plaques in the coronary arteries.
Prinzmetal angina is a condition where myocardial ischemia is caused by vasospasm of the
smooth muscle in the coronary arteries. The chest pain associated with this type of angina is not
correlated to activity but resolves quickly.
MI
Myocardial infarction occurs as a result of occlusion of a coronary artery, usually as a result of
the rupture of atherosclerotic plaque causing a thrombus. Other causes can be vasospasm,
emboli (from AF) and others…
find more resources at oneclass.com
find more resources at oneclass.com

It is usually the left coronary artery that becomes occluded as it is larger than the right. RCA
origin of infarct has an atypical presentation. Most common presentations are LAD > RCA > LCX.
There are two types of MI depth; trans-mural (full thickness necrosis) or subendocardial infarct
(less severe). Damage that occurs in the first 20 minutes of infarct are reversible however after
20 minutes the damage becomes permanent.
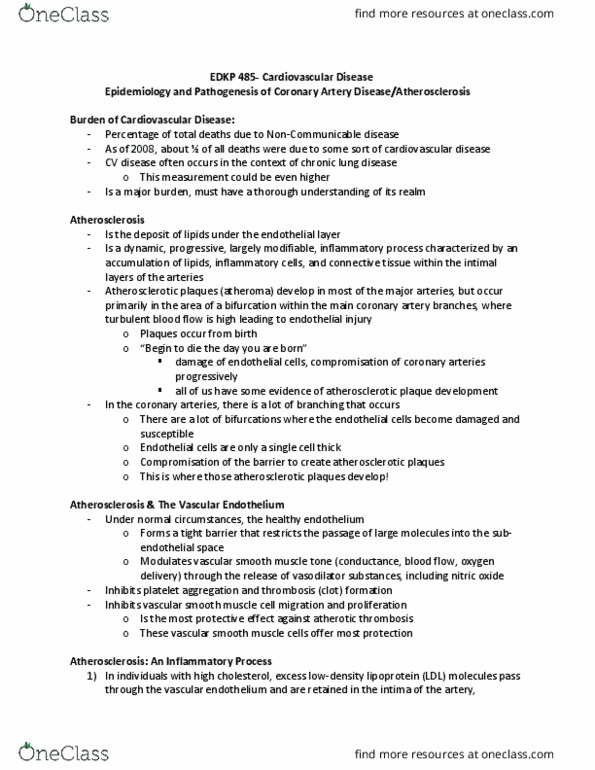
LAD Transmural Infarct
LCX Subendocardial Infarct
Myocardial Response to Ischaemia:
Within seconds – switch the anaerobic glycolysis
< 2 minutes – loss of contractility
1-10 minutes – reversible damage
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Endothelial injury and dysfunction , causing (among other things) increased vascular permeability, leukocyte adhesion, and thrombosis. Accumulation of lipoproteins (mainly ldl and its oxidized forms) in the vessel wall. Monocyte adhesion to the endothelium , followed by migration into the intima and transformation into macrophages and foam cells. Factor release from activated platelets, macrophages, and vascular wall cells, inducing smooth muscle cell recruitment, either from the media or from circulating precursors. Smooth muscle cell proliferation, extracellular matrix production , and recruitment of t cells. Lipid accumulation both extracellularly and within cells (macrophages and smooth muscle cell) Cad is atherosclerosis of the coronary arteries and is the commonest cause of mi and angina. Ihd is a group of conditions which cause ischemia to the heart; namely angina and mi. Angina is the condition associated with ischemia to the heart which does not result in infarction. There are three types of angina; stable, unstable and prinzmetal.