MEDI7111 Lecture 16: renal 16


Chronic Kidney Disease
Epidemiology
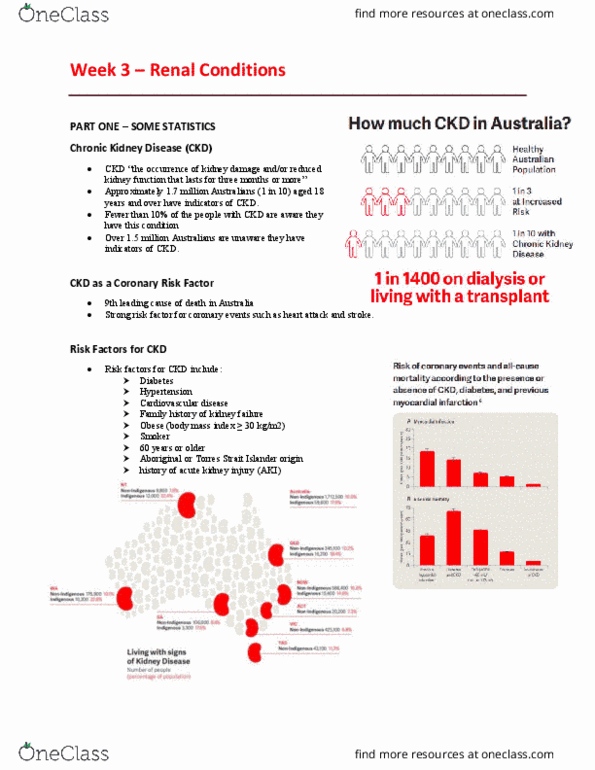
Chronic kidney disease affects 1.7 million Australians and is responsible for ~13% of deaths
annually (9th leading cause of death). 1 in 3 adults are at risk of CKD and 1 in 10 have the
condition however only 1 in 16 people with CKD are aware they have it. Each day, 6 people
begin renal replacement therapy (RRT) which is a massive financial burden to the health
budget ($600 million).
Risk Factors
Modifiable
oDiabetes
oHypertension
oObesity
oSmoking
oCVD
Non-Modifiable
oAge >60 years
oFHx of CKD
oEstablished CVD
find more resources at oneclass.com
find more resources at oneclass.com

oAboriginal or TSI person
Urban Indigenous (2x risk)
Rural Indigenous (6x risk)
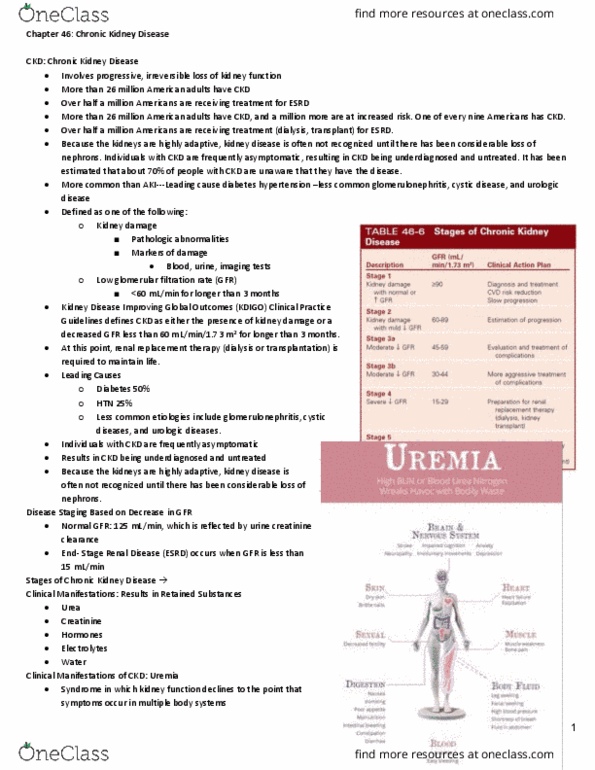
*Proteinuria/albuminuria and reduced eGFR are strong independent risk factors for CVD. A
diagnosis with CKD increases the risk of CVD 20 fold.
Aetiology & Pathophysiology
There are many causes of CKD however the most common are diabetic nephropathy and
hypertensive nephropathy, with others including structural deformities to the kidney (e.g.
hydronephrosis, PKD etc.). The pathophysiology of the disease is dependent on its aetiology.
Clinical Features
Initially, renal failure has no specific symptomology and symptoms do not present until
stage 3 renal failure. CKD is typically identified through BP monitoring, UACR and eGFR as a
result of risk factor identification, however occasionally patients will present with stage 3
symptoms.
Stage 1 & 2 Stage 3 Stage 4 Stage 5
No symptoms None
OR
Mild malaise
Nocturia
Anorexia
None
OR
Malaise
Nocturia
Anorexia
Nausea
Pruritis
Restless legs
Dyspnoea
Malaise
Nocturia
Anorexia
Nausea
Vomiting
Pruritis
Restless legs
Dyspnoea
Diagnosis
All that is required to diagnose is eGFR and UACR (urine albumin creatinine ratio). This is
more effective at diagnosis than clinical reasoning. NB - CKD-EPI eGFR is the best measure
of eGFR. If the patient has a negative test for CKD, the tests (UACR, eGFR and BP) should be
performed yearly to screen for the disease again.
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Chronic kidney disease affects 1. 7 million australians and is responsible for ~13% of deaths annually (9th leading cause of death). 1 in 3 adults are at risk of ckd and 1 in 10 have the condition however only 1 in 16 people with ckd are aware they have it. Each day, 6 people begin renal replacement therapy (rrt) which is a massive financial burden to the health budget ( million). Modifiable: diabetes, hypertension, obesity, smoking, cvd. Non-modifiable: age >60 years, fhx of ckd, established cvd, aboriginal or tsi person. *proteinuria/albuminuria and reduced egfr are strong independent risk factors for cvd. A diagnosis with ckd increases the risk of cvd 20 fold. There are many causes of ckd however the most common are diabetic nephropathy and hypertensive nephropathy, with others including structural deformities to the kidney (e. g. hydronephrosis, pkd etc. ). The pathophysiology of the disease is dependent on its aetiology.