8977 Lecture Notes - Lecture 6: Biceps, Tendinopathy, Genu Valgum

3 Jul 2018
School
Department
Course
Professor

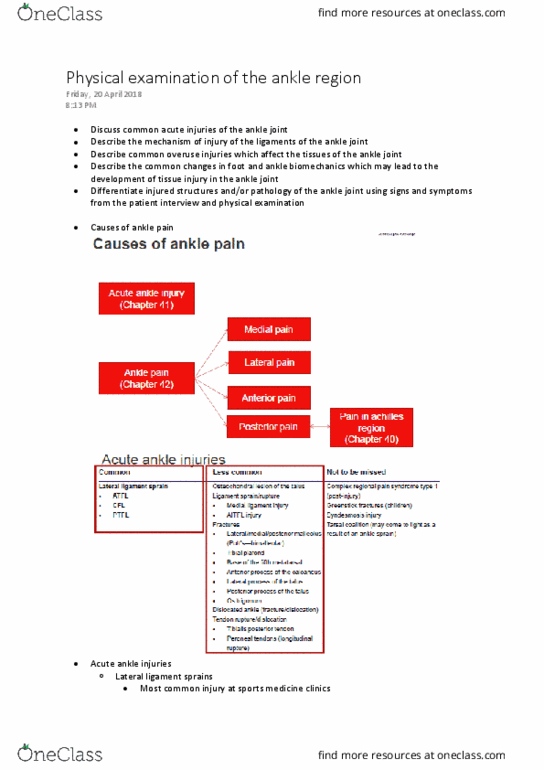
ACUTE ANKLE INJURIES
LESS COMMON
Description
Mechanism/Onset
Clinical Features
Tests
Treatment/Evaluation
OSTEOCHONDRAL
LESION OF THE TALUS
Commonly occurs in
association w ankle sprain esp.
when there is a compressive
component
Ankle sprain, during the
compressive component of an
inversion injury. Lateral=
Inversion + DF
Medial= Inversion + PF or
atraumatic
Acute or Chronic
Aching, pain, swelling stiffness, sharp
pain and can have catching or locking.
Reduced ROM, Tenderness on Talar
dome. Chronic osteochondral lesions/
osteochondritis dissecans can present
similar to arthritis ie. Crepitus, stiffness,
recurrent swelling with activity.
X-a doest alas sho,
MRI or Isotopic bone scan (+ve
bone scan should be
supplemented w a CT scan)
Stage 1: Compression # of
subchondral bone
Stage 2: Partial osteochondral
fragment #
Stage 3: Detached fragment
without displacement
Stage 4: Detached and
displaced
Put foot in plantar flexion and 45O
external rotation and feel talar surface, if
pain then may be indicative of lesion.
Stage I II can generally be treated
conservatively with 6wks in non WB cast.
Stage III and IV lesions and persistent
symptoms are treated surgically-
arthroscopy, subchondral bone drilling,
ORIF
MEDIAL LIGAMENT
INJURY
Less common than lateral, both
can occur in same sprain,
return to activity is normally
twice as long
Eversion, normally need high
force
Swelling, pain, fracture of medial
malleolus
MRI, Palpation of ligaments
(Talar Tilt eversion, DF/IR/Ev
PF/ER/Ev)
As for Lateral Ligament Sprain
ANTEROINFERIOR
TIBIOFIBULAR LIGAMENT
(AITFL) INJURY
Can be damaged during severe
ankle sprains and can be
associated w Masionneuve
fracture
Compression and eversion, acute
dorsiflexion (described as
Upward and Outward)
Maximal tenderness over AITFL, pain
and swelling
Dorsiflexion and rotation may
reproduce pain. Weight-
bearing x-ray to detect
Orthopaedic referral is necessary to
determine if fixation is required
POTTS FRACTURE
(LATERAL, MEDIAL,
POSTERIOR MALLEOLUS
FRACTURE)
Affects one or more of malleoli
can be difficult to distinguish
between sever lig sprain
Inversion
Severe pain, inability to weight bear,
swelling, bruising
Gentle palpation can generally
localize to either malleoli
(fracture) or just distal (sprain).
X-ray (use Ottawa rules)
Restore normal anatomy, Stable: use of
crutches and early mobilization,
Unstable: conservative w plaster.
LESS COMMON
Description
Mechanism/Onset
Clinical Features
Tests
Treatment/Evaluation
COMMON
Description
Mechanism/Onset
Clinical features
Tests
Treatment/Evaluation
LATERAL LIGAMENT
SPRAIN (ATFL/PTFL/
CFL)
Occurs in activities that require
rapid changes in direction, esp.
on uneven surfaces (Eg
Basketball, volleyball and
netball
Inversion and plantarflexion –
normally damages the ATFL
before the CFL
Swelling, Bruising, audible
snap/crack/tear
MRI, Anterior Draw Test, Talus
Tilt Inversion, Proprioception
Problem Ankle
G1 – no abnormal laxity
G2- some laxity w firm end point
G3- gross laxity w/out a discernible end point
Treatment: Decrease pain and swelling
(PRICEMEM protected mobilization),
increase ROM (within pain limits), strength
and Proprioception till can return to sport.
find more resources at oneclass.com
find more resources at oneclass.com

cont
TIBIAL PLAFOND
FRACTURE
Found in Skiers. Found in 7 -
10% of all tibial fractures. May
complicate a straightforward
ankle sprain
Vertical compression force. High
energy trauma
Pain, swelling, deformity, crepitus
about the ankle, inability to weight
bear
x-ray is generally normal so
MRI/CT or isotopic bone scan
are necessary
Arthroscopic debridement treatment of
choice. Look out for compartment
syndrome, compression of vertebrae,
osteoarthritis, cartilage damage
FRACTURE TO BASE
OF 5TH MT
(AVULSION OR JONES
FRACTURE) – (ALSO IN
FOREFOOT PAIN)
Most commonly avulsion
fracture. 3 zones the fracture
can occur in. Fracture of the
diaphasis (Jones). Found in
recreational and competitive
athletes
Inversion injury causes an
avulsion fraction. Normally
accompanied by a lateral
ligament sprain. Jones is an
overuse injury
Tenderness over base of 5th MT,
swelling, bruising
X-ray (needs to be looked at
carefully)
Conservatively w immobilization for 2
weeks. Will need surgery if the fracture
is displaced
# ANTERIOR PROCESS
OF THE CALCANEUS
Fractures may cause persistent
pain post sprain, occurs in 15%
in all calcaneal fractures.
Articulates with cuboid,
attached by interosseous lig.
And also the bifurcate which
attaches to both navicular and
cuboid.
Result from compression or
avulsion Compressive forces
w/out forced dorsiflexion causes
compressive # as ant. Process is
pressed against cuboid (often
intra-articular). Inversion, PF can
cause avulsion injury to calcaneus
(extra-articular).
Pain while walking, point tenderness at
calcaneocuboid joint (aprox 1cm
below, 3-4cm anterior to lateral mall),
oedema, ecchymosis, deformity of heel
or plantar arch.
X-ray w oblique foot views. If
no fracture is seen then isotopic
bone scan or MRI/CT is
indicated. Palpation can help
differentially diagnose # or
lateral lig sprain.
Small Fracture: Treat the symptoms/
protected WB
Large fracture: 4-6 weeks of non-weight-
bearing cast immobilization or surgical
excision of the fragment.
# LATERAL PROCESS
OF THE TALUS
Articulates superolaterally with
fibula, it helps to stabilise the
ankle mortise and
inferiomedially with calcaneus.
Dorsiflexion and inversion/
shearing stress or direct trauma.
Ankle pain, swelling, inability to
weight-bear, bruising, tenderness on
malleolus. Pain with PF, DF and
subtalar joint movement.
X-ray or CT scan also point
tenderness on palpation (can be
palpated anterior and inferior
to medial malleolus)
Non-displaced: short leg cast for 4-6wks,
followed by 2 wks in a walking cast and
initiation of rehab focussing on joint
stiffness and weakness. (Displaced less
than 2mm). Large displaced #s surgical
reduction and fixation is required.
#POSTERIOR PROCESS
OF TALUS
Posterior process of talus is
composed of medial ptubercle
and lateral tubercle. Lateral
tubercle serves as the
attachment for PTFL and
posterior talocalcaneal lig.
Medial tubercle as attachment
site for post. 1/3 of deltoid lig.
Inversion or when ankle is forced
into extreme equinus.
Lateral tubercle #= hyperPF or
inversion (seen in kicking sports)
Medial tubercle= DF, pronation
injuries because medial tubercle
is avulsed by deltoid lig.
Pain on posterolateral ankle. Pain on
PF and can be accentuated with DF of
big toe (# compressed by FHL tendon
as it passed between the tubercles)
With Medial tubercle # there may only
be slight pain with ambulation
decreased and painful ROM. Swelling
post. To medial malleolus, anterior to
Achilles tendon.
MRI, CT or x-ray
May require 6 weeks of immobilisation
followed by WB as tolerated. Larger and
more displaced #s required ORIF
DISLOCATED ANKLE
Falling down stairs, twisting and
impact
Pain, deformity, swelling, inability to
weight bear, tenderness on palpation
Visual observation
X-ray
Relocate as soon as possible to delay
damage to surrounding tissue
find more resources at oneclass.com
find more resources at oneclass.com

LESS COMMON
cont
Description
Mechanism/Onset
Clinical Features
Tests
Treatment/Evaluation
TIBIALIS POSTERIOR
TENDON (TPT)
RUPTURE
Usually occurs in Athletes.
Occurs w dorsiflexion and
inversion
Pain in region of navicular turborisity
extending to the posterosuperior
boarder of medial malleolus and
posteromedial tibial boarder.
Thickening/absence of the TPT.
Flattened medial arch
MRI is the investigation of
choice.
Ultrasound may be
useful.
Surgical repair is essential to maintain the
normal medial arch of the foot.
TIBIALIS POSTERIOR
TENDON
DISLOCATION
Extremely rare in sport
Occurs w dorsiflexion and
inversion. Strong contraction of
the tibialis posterior muscle pulls
the tendon out of its retinaculum
using the malleolus as a fulcrum
Moderate, not exquisite medial ankle
pain, inability to weight bear. Swelling
and bruising. Tendon can be subluxed
anteriorly and relocated posteriorly w
foot in full plantarflexion
Clinical examination but
ultrasound or MRI may
show fluid retention
Immediate surgical treatment to relocate the
tendon and repair the flexor retinaculum and
reattach the tibialis posterior sheath. Post-op
ankle is immobilized in cast for 6wks NWB.
Post cast removal can use braces. WB can
commence 6 weeks w PT supervision
PERONEAL TENDONS
(LONGITUDINAL
RUPTURE)
DISLOCATION/SUBLUX
ATION
Occurs in skiers when they
catch their toe. Once the
retinaculum is torn recurrent
dislocations can occur. Affects
young athletes. Difficult in early
stages to distinguish between
lateral lig. sprain.
Forceful passive dorsiflexion.
Retinaculum is ripped off the
posterior edge of the lateral
malleolus.
Tender peroneal tendons that can be
dislocated by PT esp. in forceful DF and
eversion. Pain at posterior distal fibula,
swelling, ecchymosis and
apprehension/inability to evert the
foot against resistance. Lateral ankle
poppig sappig ad istailit is
reported.
Palpation of the Tendons
during objective
examination and a
negative anterior draw is
diagnostic of peroneal
tendon subluxation.
Surgical repairment of the tendons in the
peroneal groove and repair of the retinaculum
using bone anchors or drill holes. If the groove
is shallow a deepening of the groove or
rotation of the malleolus may also happen.
Soft tissue repair also produces good results
# OS TRIGONUM
Found on posterior surface of
Calcaneus posterior to lateral
tubercle. Occurs ~10% of popn,
often unilateral. Origin may be
congenital (separation of
2ndary ossification centre) or
acquired(2ndary to actual
fracture)
Acute plantarflexion injury in
kicking
Pain posteriorly with max
plantarflexion
X-ray/MRI
Symptom reduction with restoration of normal
strength, ROM & biomechanics as needed.
May require surgical excision (after skeletal
maturity is reached)
NTBM
Description
Mechanism/Onset
Clinical Features
Tests
Treatment/Evaluation
COMPLEX REGIONAL
PAIN SYNDROME TYPE
1
Formally known as RSD.
Associated w regional
osteoclast overactivity
Usually occurs post trauma
Severe regional pain, swelling,
dysesthesia to light touch (allodynia)
and vasomotor instability. Pain is out of
proportion to the degree of injury
x-ray to show regions of
patchy demineralization
or bone scan showing
increased areas of uptake
If pain does not settle, chemical or surgical
blockade is indicated. Very hard to treat
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Occurs in activities that require rapid changes in direction, esp. on uneven surfaces (eg. Inversion and plantarflexion normally damages the atfl before the cfl. G3- gross laxity w/out a discernible end point. Treatment: decrease pain and swelling (pricemem protected mobilization), increase rom (within pain limits), strength and proprioception till can return to sport. Commonly occurs in association w ankle sprain esp. when there is a compressive component. Ankle sprain, during the compressive component of an inversion injury. Aching, pain, swelling stiffness, sharp pain and can have catching or locking. Chronic osteochondral lesions/ osteochondritis dissecans can present similar to arthritis ie. crepitus, stiffness, recurrent swelling with activity. Less common than lateral, both can occur in same sprain, return to activity is normally twice as long. Mri or isotopic bone scan (+ve bone scan should be supplemented w a ct scan) Mri, palpation of ligaments (talar tilt eversion, df/ir/ev.