HUBS1403 Lecture 34: Lecture 34- Cardiac and Smooth Muscle

8 Jun 2018
School
Department
Course
Professor
Cardiac and Smooth
Introduction to the heart
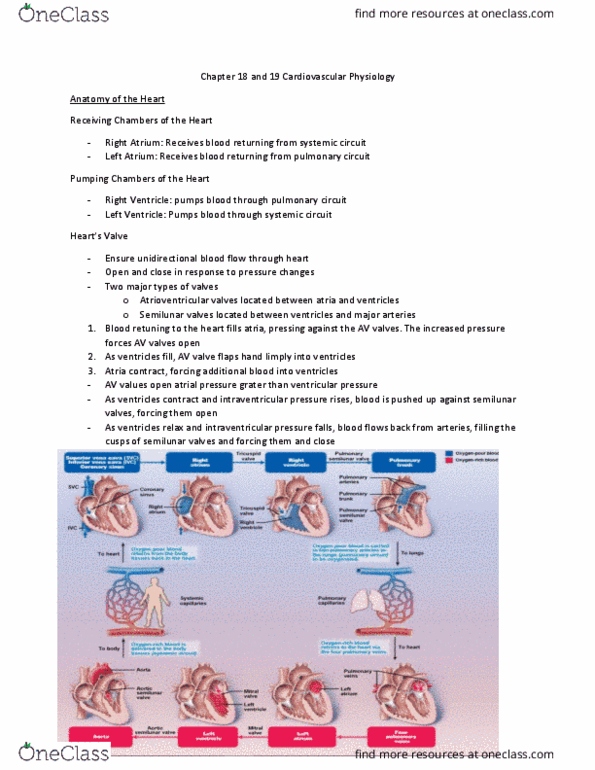
• Heart is a double pump
• Blood has to first fill the chamber (ventricle) before it can be pumped from it
Both sides (pumps) have to be co-ordinated in pumping action - achieved by coordinated electrical
signalling
Cardiac Muscle Features
Skeletal muscles were large cells, tendon to tendon driven by AP
Cardiac muscle cells are different:
• 20uM diameter and 50-100uM long
• They are mononucleated and joined by intercalated discs - cope with rigors of contraction
• Cells do not multiply so they have to last a lifetime - heart damage is serious
o It had been found that prenatal babies in the womb can repair their heart cells
• Cardiac has length tension relationship but smooth must be different
Cardiac Muscle Activity
Unlike skeletal muscle, contraction is initiated by pacemaker cells
Light muscle - in atrium because of its staging point
Strong muscle - In ventricle because they must push blood through the body
Left ventricle - more muscled because body has more resistance than lungs
• Unlike skeletal muscle, cardiac AP is triggered by pacemaker cells
• AP signal for contraction initiated in the SA node and is conducted through the heart by
specialised muscle cells called purkinje cells
• Conducting system. These are specialised muscle cells (purkinje) that behave more like
neurons and have very little contractile purposes
• Every single cell has the ability to beat - they only beat in synchrony because they are together
o They receive signals from other cells and SA node to coordinate the beating
• SA node beats at about 60bpm - if it gets damaged:
o AV node will continue to beat at 40bpm -if it then gets damaged:
o Ventricular cells continue to beat at 20bpm
o So all the cells will continue to beat - not at an ideal rate though
• Atria first then ventricles
• Pacemaker is the SA node in the right atrium that initial contraction style of heart
• They are pacemakers because they are the fastest cycle time, ventricle cells can beat
spontaneously but slower (every cells has beating properties)
Hierarchy of peacemaking:
• SA node resents clock in ventricle - refractory period
• Ectopic (out of place) contractions - when ventricle cells beat to fast
Aps in SA Node Pacemaker Cells
• Na channel for upstroke - always open
• K channel for downstroke
Similar to the neuronal AP but with some key difference
1. AP is very slow compared to neurons (different types of K channels)
2. PD does not rest like a neuron, is climbs (depolarises) spontaneously
Depolarisation is due to Na current and due to Na Ca exchanger which increases pace making during
exercise
• Leads to 75bpm for rest
• 45bpm for trained athletes
Autonomic Inputs Modulate Pacemaker Activity
parasympathetic input slows pacemaker activity
• What is working most of the time when at rest

Parasympathetic neurons use Ach to open K channels. Slows and extends hyperpolarisation of
membrane. Longer to get to threshold
Sympathetic input accelerates pacemaker activity
Sympathetic neurons release adrenaline which acts on receptors that lead to opening of Na
channels, this causes the opposite effect
Also ca2+ release from SR which has a clock cycle
Thus, neural inputs do not initiate cardiac contractions, but they can modulate them
• Each AP sets off a heart contraction
More Na - reach threshold earlier - more Aps - increase in HR
Neural inputs alter the rate of pacemaking in the SA node
• Threshold at -40mV in all panels
• Other line at -60mV
Active Process: HR without neuronal input is about 100bpm
Pacemaker Aps spread via gap junctions
Another difference between skeletal and cardiac muscle cells are their size:
• Cardiac cells are 20um diameter and 100um long
• They are joined at intercalated discs by 2 structures
o Desmosomes hold together - withstands rigors
o Gap junctions (large diameter channels;) give an electrical connection by allowing ions to
flow
• Transmission of signal occurs from cell to cell through gap junctions - unique to cardiac muscle
AP in non-pacemaker cardiac muscle fibres
• Occurs in ventricle
• Ions that underlie AP here are quite like in a neuron - but much slower
o Voltage gated K channels - take a while to open - but bring AP back down again
• There is a refractory period (important!)- Na channels are paralysed until the
hyperpolarisation finishes
• This helps the heart not to have summation of contractions - regular beat
Timing of contractions in cardiac vs skeletal muscle
• Aps of "ordinary" cardiac muscle cells differ from both pacemaker and skeletal muscle Aps
• Key difference between cardiac and skeletal muscle AP is the duration of AP relative to
contraction, and thus the refractory period - prevents tetanus in cardiac muscle
Skeletal muscle: Contraction can happen during refraction
Cardiac Muscle: Contractions must be after refraction
Note: resting PD more negative than in pacemaker cells --- slower
• The timing of muscle contraction is very different in cardiac and skeletal muscles
• This is in contrast to skeletal muscle where summation occurs, contraction after refraction
• Duration of AP is much longer in cardiac - due to slower K channels
o Skeletal AP is more like a neuron
• Hence Abs refractory period and relative refractory period is much longer
o Cardiac muscle can't have another beat during contraction
o This gives time for the blood to flow
• When AP is too long the refractory period interferes with the next excitation
• When AP is too short tissue can excite again before the next heart beat (reentrant)
Structural Features of Cardiac Muscle Cells
• Smaller than skeletal muscle cells (max 20 x 100um)
• Single nucleus
Document Summary
Introduction to the heart: heart is a double pump, blood has to first fill the chamber (ventricle) before it can be pumped from it. Both sides (pumps) have to be co-ordinated in pumping action - achieved by coordinated electrical signalling. Skeletal muscles were large cells, tendon to tendon driven by ap. 20um diameter and 50-100um long: they are mononucleated and joined by intercalated discs - cope with rigors of contraction, cells do not multiply so they have to last a lifetime - heart damage is serious. It had been found that prenatal babies in the womb can repair their heart cells: cardiac has length tension relationship but smooth must be different. Unlike skeletal muscle, contraction is initiated by pacemaker cells. Light muscle - in atrium because of its staging point. Strong muscle - in ventricle because they must push blood through the body.