BMS1052 Lecture Notes - Lecture 27: Retinitis Pigmentosa, Deep Brain Stimulation, Indirect Pathway Of Movement

5 May 2018
School
Department
Course
Professor

Lecture 25,26 printed out
Lecture 27- Bionics and neural prosthetics
Lecture objectives
- describe the possible mechanisms by which Deep Brain Stimulation may provide
relief from symptoms of Parkinsons disease
- Describe the symptoms of retinitis pigmentosa and macular degeneration
- Describe the relative advantages of cortical and retinal stimulation for producing a
visual prosthesis
- Describe the challenges involved in recording and decoding EMG and cortical signals
in order to control a motor prosthesis
• Sensory
– Auditory
– Visual
– Pain relief
• Motor
– Controlling movement
– Bladder control
• Cognitive
– Parkiso’s disease
– Depression
– Mid readig
Parkinson’s disease
PD is characterised by loss of dopaminergic neurons in the SNc
- Loss of dopaminergic cells leads to increased inhibition
of thalamic Vlo, reduced cortical activation and hypokinesia
Symptoms
- resting tremor
- shuffling gait
- akinesia – impaired initiation of movement
- bradykinesia – reduced amplitude / velocity of voluntary movement
- advanced symptoms – cognitive impairment, dementia
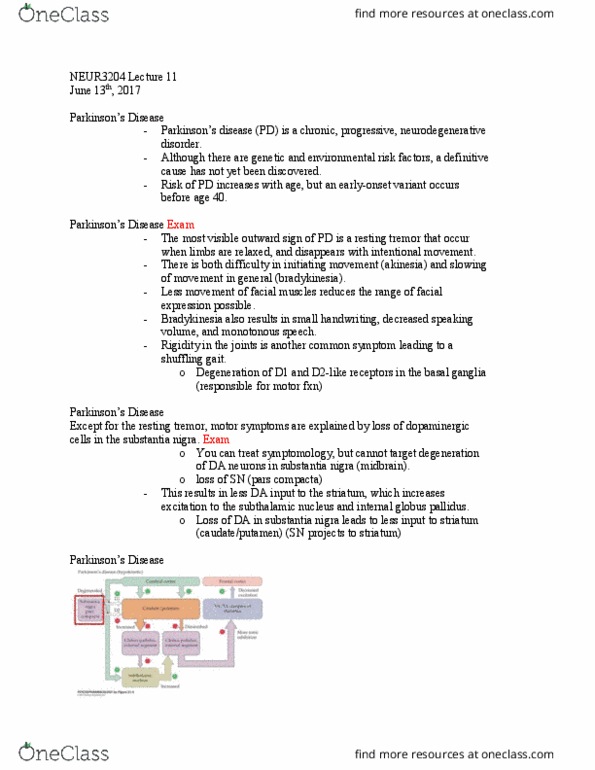
1. Direct pathway facilitates selection of a movement plan in cortex
2. Indirect pathway inhibits movement selection
3. Dopaminergic projections from SNc to striatum excite direct and inhibit indirect
pathway
4. Loss of dopaminergic SNc neurons accounts for PD symptoms
find more resources at oneclass.com
find more resources at oneclass.com

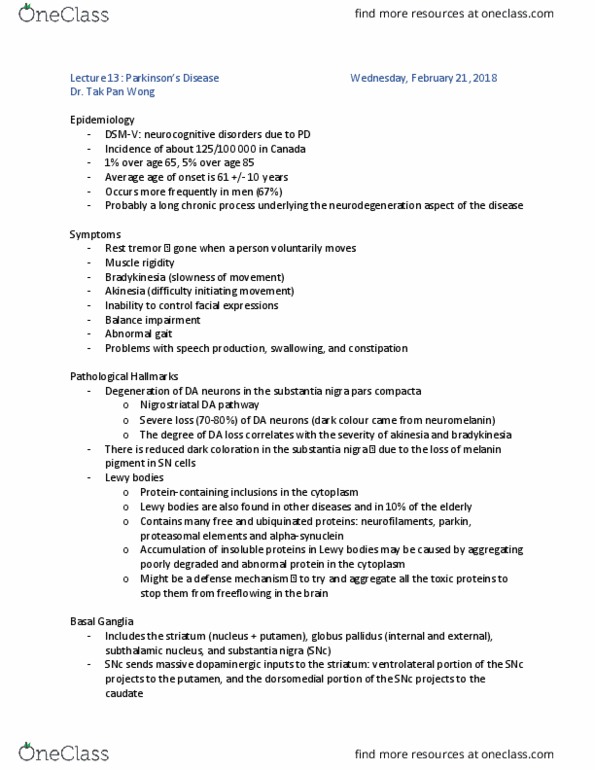
Surgical treatment for Parkinsons Disease:
- Remove STN or GPi
How does this affect the circuit?
Surgical approach is to remove STN or Gpi
Gpi directly inhibits Vlo, and since STN is excitatory, increased activity in STN also leads to
inhibition of VLo.
Thus, removing these areas reduces the inhibition of VLo, leading to increased cortical
activity.
Can be side-effects – imbalance in ability to initiate movement can swing too far in the
other direction, leading to hyperkinesia and generation of unwanted movements.
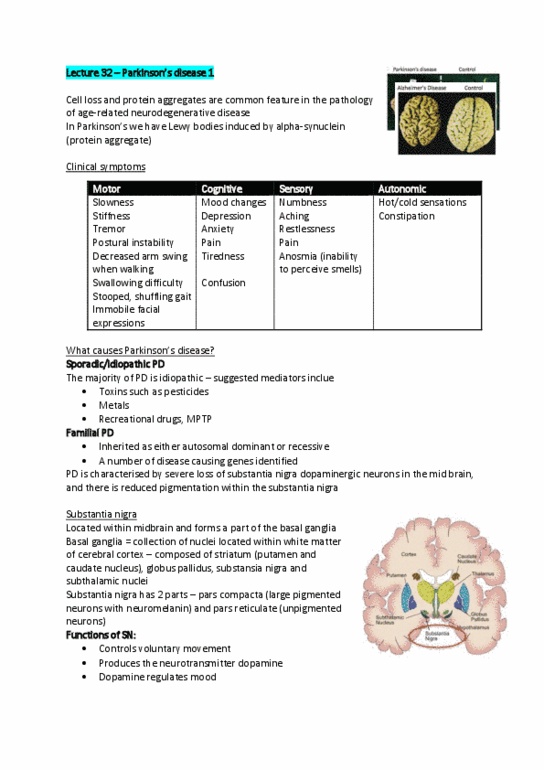
Deep brain simulation
- unlike a surgical lesion, electrical stimulation is reversible and controllable
- Only used when symptoms are not controlled by medication
- stiulatio is like a rai paeaker – chronic, low frequency stimulation of STN or Gpi
DBS- The most likely neural mechanism is chronic inhibition
• Stimulation of STN or GPi can reduce PD symptoms
• DBS produces similar effects to lesion
Chronic stimulation inhibits the local region
DBS- Exact neural mechanisms are unclear
• Effects of stimulation may be mediated at level of afferent axons, cell bodies,
efferent axons or astrocytes
• DBS may modulate firing rates
• DBS may normalise irregular burst firing rates
• DBS may desynchronise low frequency oscillations in cortical loop
• DBS may increase adenosine release from astrocytes, depressing excitatory
transmission in the thalamus
SNc has a dopaminergic projection to striatum (like
Gpi and SNr, it receives excitatory and inhibitory
projections from striatum and STN).
There is a neat functional segregration in the
striatum, allowing dopamine to have different effects
on the striatal neurons:
- Neurons in direct pathway are excited (D1 dopamine
receptors)
- neurons in indirect pathway are inhibited (D2
dopamine receptors)
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Describe the possible mechanisms by which deep brain stimulation may provide relief from symptoms of parkinsons disease. Describe the symptoms of retinitis pigmentosa and macular degeneration. Describe the relative advantages of cortical and retinal stimulation for producing a visual prosthesis. Describe the challenges involved in recording and decoding emg and cortical signals in order to control a motor prosthesis: sensory. Pd is characterised by loss of dopaminergic neurons in the snc. Loss of dopaminergic cells leads to increased inhibition of thalamic vlo, reduced cortical activation and hypokinesia. Snc has a dopaminergic projection to striatum (like. Gpi and snr, it receives excitatory and inhibitory projections from striatum and stn). There is a neat functional segregration in the striatum, allowing dopamine to have different effects on the striatal neurons: Neurons in direct pathway are excited (d1 dopamine receptors) Neurons in indirect pathway are inhibited (d2 dopamine receptors) Surgical approach is to remove stn or gpi.