BMS2031 Lecture Notes - Lecture 10: Aquaporin, Ureter, Clinical Urine Tests

31 May 2018
School
Department
Course
Professor

Week 4. Urine formation (tubular reabsorption),
Regulation of total body water, and Regulation of
total body sodium
URINE FORMATION (TUBULAR REABSORPTION)
• Tubular reabsorption contributes to medullary hyperosmotic gradient
• Some substances are almost completely reabsorbed (many ions are highly reabsorbed) with 99%
of filtrate is taken back into the body
• Why filter then reabsorb?
o GFR is normally 125ml/min or 180l/day
o Without tubular reabsorption the whole plasma volume and essential solutes would be
excreted within 30 minutes
o What would happen in the body if glomerular filtration continued at a normal rate but
tubular reabsorption decreased to 50% of the normal rate?
- usually almost everything is reabsorbed
-normally (3000ml/125ml/min = 24) with no reabsorption you would lose all filtration in
24 minutes so if 50% of rate then you would lose everything in 48 minutes
-remember only 20% of plasma if filtered
find more resources at oneclass.com
find more resources at oneclass.com

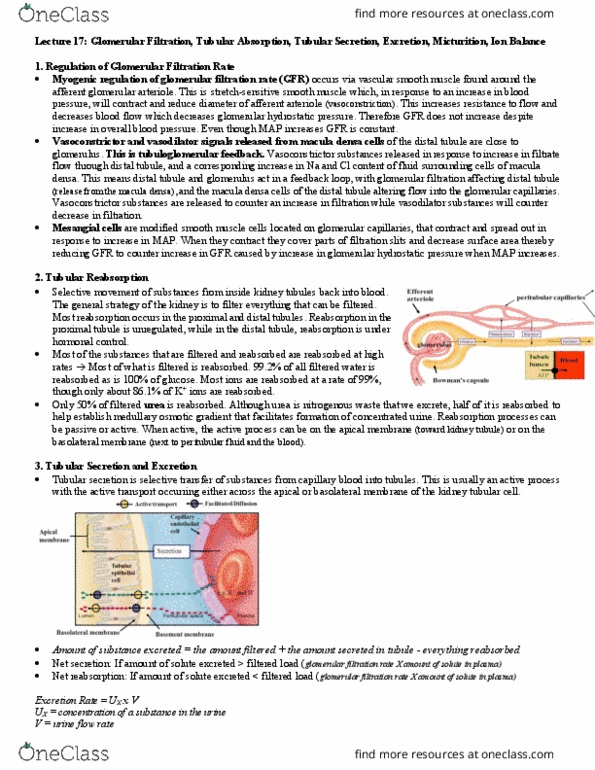
• Pathways for tubular reabsorption:
o Paracellular: through tight junctions
o Transcellular: through cells
Can be:
o Passive: simple diffusion, channel mediated, carrier mediated (eg. glucose), osmosis
o Active transportation (use ATP): primary or secondary
-> sodium
• Reabsorption of sodium and water in the renal tubules
Why? Because control of the levels of water and sodium in the body determines the
extracellular (including plasma) fluid volume and osmolarity (include blood volume and hence
MAP)
o Reabsorption of sodium is mainly an active process
o Reabsorption of water is by diffusion and is secondary to sodium (water follows the
solutes down a concentration gradient)
• Reabsorption by mediated transport:
o For substances that are actively reabsorbed, there is a limit to the rate the solute can be
transported back into the peritubular capillaries
o Due to saturation of available carrier proteins
-> excess excreted in urine
o Transport maximum (Tm; mg/min)
find more resources at oneclass.com
find more resources at oneclass.com

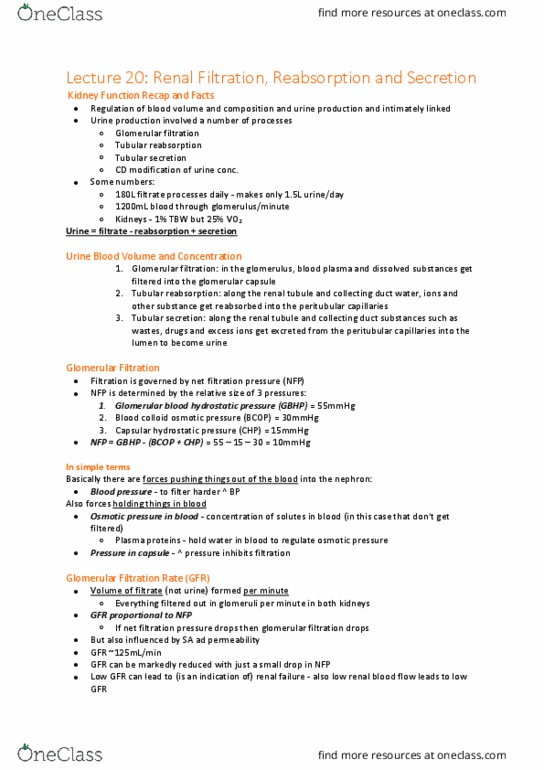
• Filtration of glucose:
o Is usually proportional to the plasma concentration until the transport maximum is
reached
o Normal Glucose plasma = 100mg/100ml
o Filtered load = glucose plasma x GFR = 100mg/100ml x 125ml/min = 125mg/min
o Tm for glucose ~375mg/min
o Renal threshold is the point where you begin to see glucose in urine (is smaller than Tm
~300, get a range of Tm hence get an overestimation)
o Glucose excretion is 0 until the renal threshold is reached
o Normal glucose range = 100-200
• Diabetes Mellitus:
o Elevated plasma glucose levels -> excreting glucose in urine
o Uncontrolled: glucose filtered load > glucose Tm = Glucosuria (glucose in urine)
• Humans usually excrete urine that is more concentrated than body fluids:
o Maximal urine concentration in human kidney = 1200 mOsmol/L
o Body fluid ~300mOsmol/L
o Typical daily excretion of solutes ~600 mOsmol/day with minimum volume of water for
solute = 0.5L/day
• We can concentrate urine (hyperosmotic) due to the medullary interstitial hyperosmotic
gradient
• Two types of nephrons:
Cortical nephrons
Juxtamedullary nephrons
o Have glomerulus in cortex of kidney
o Short loop of henle which barely protrudes
into outer medulla
o No vasa recta
o Have glomerulus sitting just next to border
between medulla and cortex
o Long loops of henles that protrude down
into inner medullary zone
o Loop of henle is associated with specialised
blood vessels called vasa recta (counter-
current exchanger)
-> maintains hyperosmotic gradient
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Regulation of total body water, and regulation of total body sodium. Normally (3000ml/125ml/min = 24) with no reabsorption you would lose all filtration in. 24 minutes so if 50% of rate then you would lose everything in 48 minutes. Remember only 20% of plasma if filtered: pathways for tubular reabsorption, paracellular: through tight junctions, transcellular: through cells. Can be: passive: simple diffusion, channel mediated, carrier mediated (eg. glucose), osmosis, active transportation (use atp): primary or secondary. > sodium: reabsorption of sodium and water in the renal tubules. Because control of the levels of water and sodium in the body determines the extracellular (including plasma) fluid volume and osmolarity (include blood volume and hence. > excess excreted in urine: transport maximum (tm; mg/min, filtration of glucose: Cortical nephrons: have glomerulus in cortex of kidney, short loop of henle which barely protrudes into outer medulla, no vasa recta.