BIOLOGY 2F03 Lecture Notes - Lecture 3: Capillary Refill, Cerebral Edema, Listeria Monocytogenes

19 May 2018
School
Department
Course
Professor

Meningitis
• Confirmed by inflammatory cells in the CSF
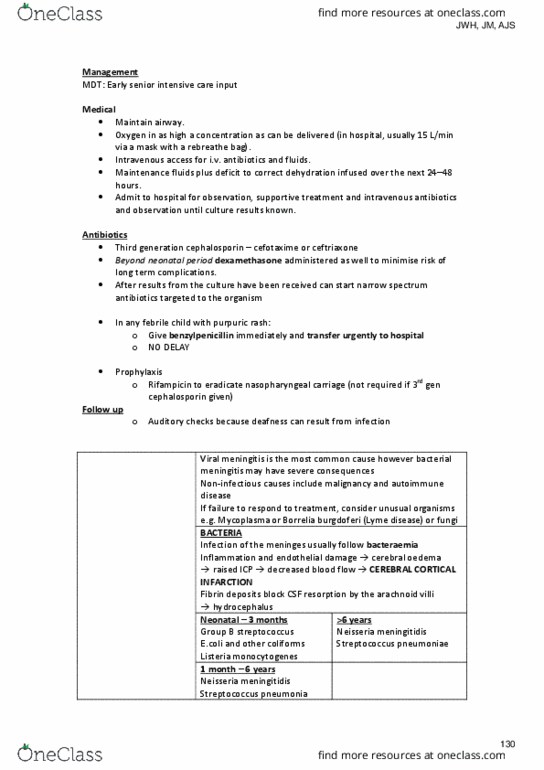
• Causes: viral are most common and are self-resolving. Bacterial may have severe consequences. Other
causes of meningitis inc: malignancy + autoimm diseases.
Bacterial Meningitis
• Usually follows bacteraemia.
• Host response to infection causes most damage.
• Inflam mediators, activated leucocytes & endothelial damage cause cerebral oedema, IC press and
cerebral blood flow.
• Organisms:
o < 3 Months: group B strep, E.coli, coliforms, Listeria monocytogenes
o < 6yrs: Neisseria meningitidis (meningococcus), strep pneumoniae, H. influenzae
o >6yrs: Neisseria meningitidis, strep pneumoniae
• Presentation:
o Meningeal signs: stiff neck, photophobia, opisthotonos
o IC press: irritable, high-pitch cry, drowsy, vomiting, fontanelle tense (late sign)
o Septic signs: fever, arthritis, odd behaviour, purpuric rash (in meningococcus), cyanosis, DIC, ++WCC
o Shock: tachycardic, hypotensive, poor capillary refill time, oliguria
• Ix: CSF (confirms Dx, identifies organism + AB sensitivity). Bloods, throat swab, rash scraping
• Rx:
o 3rd generation cephlosporin (cephotaxime or ceftriaxone).
o Ampicillin in <3/12 olds
o Dexamethasone reduces long-term complications
• Complications:
o Hearing loss
o Subdural effusions
o Disseminated disease
o Hydroencephalus
o Brain abscess
o Paralysis
o Ataxia
o Mental retardation
o Epilepsy
Cerebral Palsy
• Comprises a range of chronic disorders of posture and movement caused by non-progressive CNS lesion
sustained before 2 yrs old, resulting in delayed motor development, evolving CNS signs +/- learning
disability +/- epilepsy.
• Causes:
o Antenatal (80%): cerebral dysgenesis + malfornation, congen inf -rubella, tox, CMV
o Intrapartum (10%): birth asphyxia/trauma
o Postnatal: IVH, meningitis, trauma.
• Clinical presentation:
o Abnormal tone and posture
o Feeding difficulties
o Delayed motor milestones
o Abnormal gait once walking
o Developmental delay (language and social skills)
Spastic (70%)
• Damage to upper motor neurone (pyramidal or corticospinal) pathway
• limb tone (spasticity), deep tendon reflexes + extensor plantar response
• distribution of signs:
o Hemiplegia
o Diplegia
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Meningitis: confirmed by inflammatory cells in the csf, causes: viral are most common and are self-resolving. Other causes of meningitis inc: malignancy + autoimm diseases. Bacterial meningitis: usually follows bacteraemia, host response to infection causes most damage, inflam mediators, activated leucocytes & endothelial damage cause cerebral oedema, ic press and. Bloods, throat swab, rash scraping: rx, 3rd generation cephlosporin (cephotaxime or ceftriaxone), ampicillin in <3/12 olds, dexamethasone reduces long-term complications, complications, hearing loss, subdural effusions, disseminated disease, hydroencephalus, brain abscess, paralysis, ataxia, mental retardation, epilepsy. Intrapartum (10%): birth asphyxia/trauma: postnatal: ivh, meningitis, trauma, clinical presentation, abnormal tone and posture, feeding difficulties, delayed motor milestones, abnormal gait once walking, developmental delay (language and social skills) Spastic (70%: damage to upper motor neurone (pyramidal or corticospinal) pathway, limb tone (spasticity), deep tendon reflexes + extensor plantar response, distribution of signs, hemiplegia, diplegia, quadreplegia.