MEDRADSC 2I03 Lecture Notes - Lecture 13: Central Venous Pressure, Internal Jugular Vein, Brachiocephalic Vein

25 Nov 2016
School
Department
Course
Professor
Document Summary
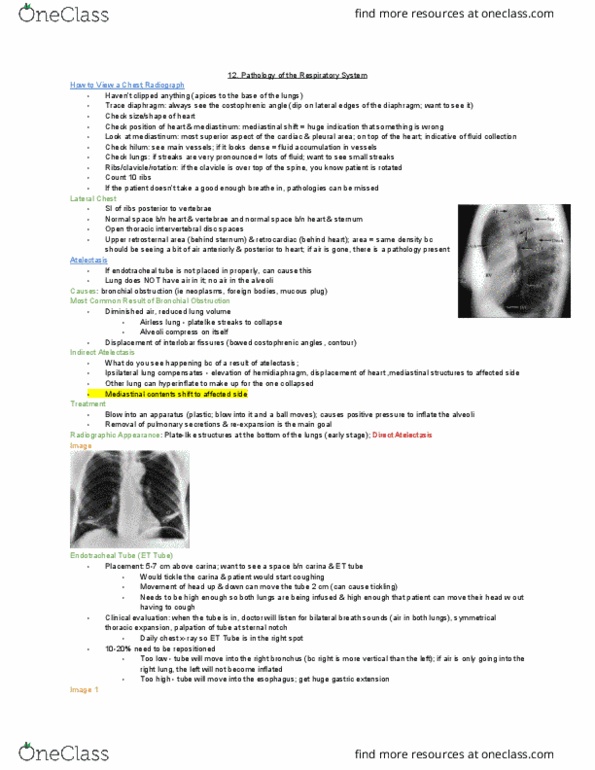
Clinical evaluation- bilateral breath sounds, symmetrical thoracic expansion, palpation of tube at sternal notch. 10 to 20 % need to be repositioned. A tube positioned too low usually extends into the right bronchus (right is more vertical) A tube positioned too high will sit in the esophagus. It has collapsed the lung, the tip is in the pleural space (not good) Inserted into subclavian or peripheral vein in upper extremity to measure central venous pressure (cvp) Portal for rapid infusion of fluids, meds or nutrition. Optimal location- where the brachiocephalic vein joins svc or within svc. 1/3 need to be reinserted- incorrect or patient motion or motion due to other tests. The most common malpositioning: internal jugular vein. Complications: right atrium- increased risk of cardiac arrhythmias and perforation; could interfere with transmission of signals, risk of pneumothorax, perivascular placement may do bad things, puncture of subclavian artery, air embolism. Longterm venous access device (saves being stabbed over and over again)