PHRM 311 Lecture Notes - Lecture 5: Sunscreen, Escitalopram, Selective Serotonin Reuptake Inhibitor

Document Summary
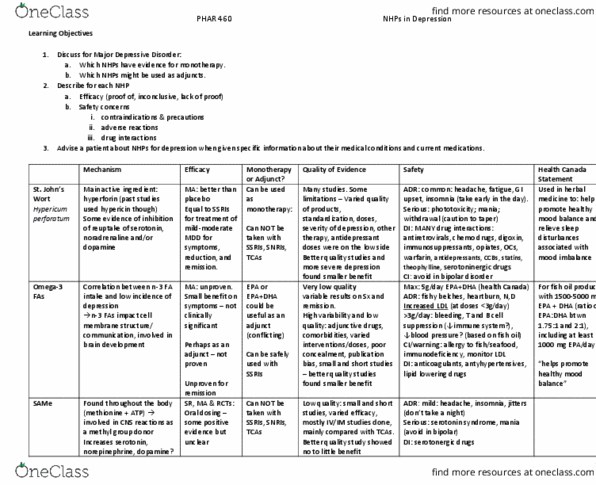
79% had not disclosed use to psychiatrist. Take home message : many plants have been studied in various psychiatric conditions. Recall the canmat guideline recommendations for the use/indication and role of sjw, Insufficient evidence to recommend n-3 monotherapy or in combo, same. Not recommended: sjw despite potential efficacy due to uncertain optimal doses, variations in preparations, potential interactions. Inhibits reuptake of 5-ht, na, da, gaba, l-glutamate. As effective as ssri treatment at ameliorating depressive symptoms. Fewer adrs than ssris and less sexual dysfunction . Common: headache, fatigue, gi upset, insomnia (take in am) Withdrawal syndrome (caution patient to taper) similar to ssris. Strong inducer of p-glycoprotein and cyp450 (mainly 3a4 ; also 1a2, 2c19, 2c9) >45 drug interactions (19 major) and any other p-glycoprotein/p450 3a4 substrates. Immunosuppressants (30-70% decrease of cyclosporin has resulted in rejection) 300 mg tid (extract standardized to 0. 3% hypericin and 2-5% hyperforin) Effect usually seen after 10-14 days (significant clinical response at 4-6 weeks )