MEDI7302 Study Guide - Final Guide: Bone Pain, Hemoptysis, Costodiaphragmatic Recess


Thoracic surgery
Learning
objectives
Identify rib fractures on imaging and list implications for underlying structures.
Recognize a pneumothorax on imaging, list causes and formulate a management
plan
Be able to recognize and institute early management of a tension pneumothorax
Discuss the pathophysiology of pleural effusions
Contrast the presentation and management of empyema and lung abscess
Form a differential diagnosis and investigative work-up of the solitary lung nodule
(‘coin lesion’)
Outline the management of non-small cell lung cancer
Rib fractures 10% all trauma patients, 30% significant chest trauma patients
# rib fractures correlates to risk of intrathoracic injury
Flail chest
2+ contiguous ribs are broken in 2+ places, moving paradoxically with
respiration
Associated injuries - pneumothorax, haemothorax, pulmonary contusion,
respiratory failure
Fracture of ribs 8-12 can damage - spleen (ribs 9-11), liver, kidneys
Management
Medical Analgesia
Respiratory support via O2 therapy, non-invasive
ventilation, intubation
Chest physio
Chest wall stabilization (if flail chest)
Treatment of complications/ associated injuries
Surgery Indications - flail chest with ventilator dependence,
significant deformity, painful fractures refractory to analgesia
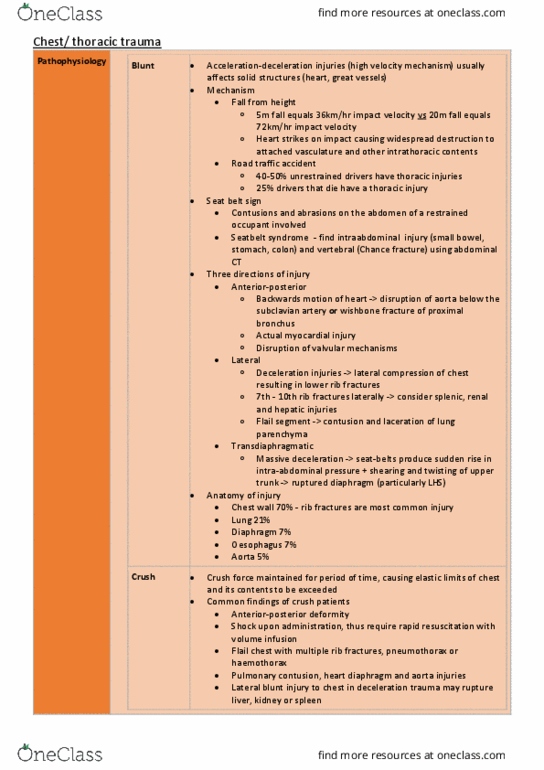
Pneumothorax Etiology
Primary - congenital subpleural blebs
Secondary - underlying lung disease (eg COPD, emphysema), trauma
Risk factors
Primary - tall thin, male, smokers (20-30x risk)
Symptoms
Dyspnoea
Pleuritic chest pain
Subcutaneous emphysema
Signs
Decreased air entry
Hyperresonant on percussion
find more resources at oneclass.com
find more resources at oneclass.com

Deviated trachea
Diagram
L sided pneumothorax
Management
Medical Small, minimally symptomatic (<2cm) - observe
Moderate - aspiration
Large - chest drain (5th IC space, lateral to pectoral
groove, anterior to mid-axillary line)
Surgery Indications - 2nd ipsilateral pneumothorax, 1st
contralateral pneumothorax, synchronous bilateral pneumothoraces, 1st
pneumothorax in professions at major risk (pilots, drivers)
Recurrence rate
1st pneumothorax = 30% recurrence chance
2nd pneumothorax = 60% recurrence chance
Continuing to smoke increases recurrence chance significantly
Tension
pneumothorax
Clinical diagnosis (not XR)
Symptoms/ signs
Respiratory distress
Haemodynamic compromise
Pneumothorax signs
Tracheal deviation
Management
Emergency - large bore IV needle compression into 2nd IC space at mid-
clavicular line
Pleural effusion Types
Transudate Exudate
Lungs
affected
Bilateral Unilateral
Etiology Systemic
factors altered
Elevated
pulmonary capillary pressure
CHF
Cirrho
sis + ascites
Hypot
hyroidism
Reduced
oncotic pressure
Hypoa
lbuminaemia (renal failure/
nephrotic syndrome)
Local factor
imbalance via leaky capillaries from
inflammation
Infection
Malignancy
RA/SLE
Oesophageal
perforation
Chlothorax
Haemothrorax
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Identify rib fractures on imaging and list implications for underlying structures. Recognize a pneumothorax on imaging, list causes and formulate a management. Be able to recognize and institute early management of a tension pneumothorax. Contrast the presentation and management of empyema and lung abscess. Form a differential diagnosis and investigative work-up of the solitary lung nodule ( coin lesion") Outline the management of non-small cell lung cancer. 10% all trauma patients, 30% significant chest trauma patients. # rib fractures correlates to risk of intrathoracic injury. 2+ contiguous ribs are broken in 2+ places, moving paradoxically with. Associated injuries - pneumothorax, haemothorax, pulmonary contusion, respiratory failure. Fracture of ribs 8-12 can damage - spleen (ribs 9-11), liver, kidneys. Respiratory support via o2 therapy, non-invasive ventilation, intubation. Pneumothorax significant deformity, painful fractures refractory to analgesia. Secondary - underlying lung disease (eg copd, emphysema), trauma. Primary - tall thin, male, smokers (20-30x risk)