PHYL2001 Study Guide - Final Guide: Perfusion, Stethoscope, Google Analytics


Cardiovascular Physiology
The Cardiovascular System:
• Functions of the cardiovascular system
o Delivery of O2, glucose and other nutrients to active tissues
o Removal of CO2, lactate and other waste products from active
tissues
o Transport of metabolites and other substances to and from storage
sites
o Transport of hormones, antibodies and other substances to site of
action
• Components of the cardiovascular system
o Arteries → accept blood from the ventricles of the heart
o Arterioles → small arteries → control flow
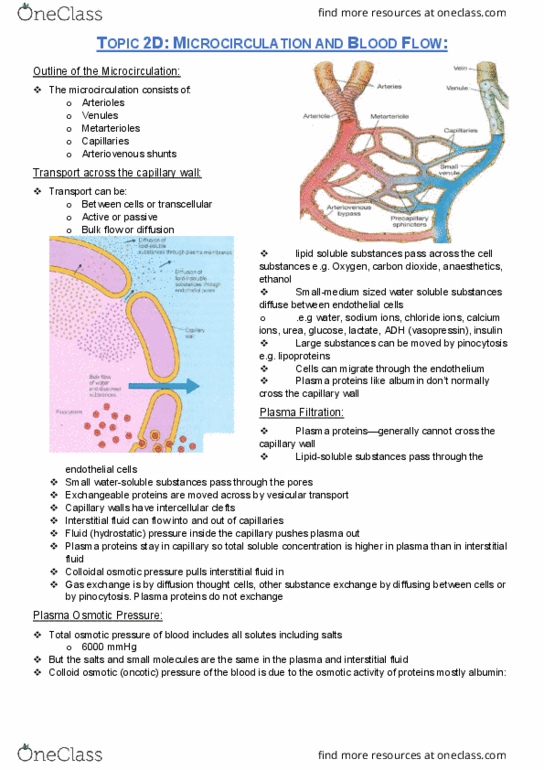
o Microcirculation → connects arterioles to venules → includes
capillaries
o Capillaries → site of exchange
o Venules → small veins → collect blood from microcirculation
o Veins → deliver blood to the atria of the heart → blood storage
vessels
• Types of circulation
o Pulmonary circulation
▪ From the right side of the heart → gains O2
▪ Pulmonary arteries → deoxygenated blood
▪ Pulmonary veins → oxygenated blood
o Systemic circulation
▪ The rest of circulation → delivers O2
▪ Systemic arteries → oxygenated blood
▪ Systemic veins → deoxygenated blood
o Systemic and pulmonary circulations are in series with each other
• Some numbers
o Diastole → relaxation of the heart
o Systole → contraction of the heart
o Diastolic pressure → 80mmHg → lowest systemic arterial
pressure during diastole
o Systolic pressure → 120mmHg → highest systemic arterial
pressure during systole
o Blood pressure → systemic arterial pressure → systolic/diastolic
→ 120/80
o Pulse pressure → 40mmHg → difference between systolic and
diastolic pressure
Cardiac Output:
• Cardiac output → amount of blood the heart pumps each minute
find more resources at oneclass.com
find more resources at oneclass.com

• 5L at rest → max. exercise = 20 L/min
• Volume pumped each minute depends on
o Number of strokes → heart rate
o Volume per stroke → stroke volume
• Heart rate → 70 beats/min → number of contractions per unit time
• Stroke volume →70-80mL → volume pumped by a ventricle in 1
contraction
• Cardiac output = heart rate x stroke volume
• Venous return → 5L/min → flow rate into the heart → controls stroke
volume
• Ventricular volumes
o End diastolic volume = 130mL
o End systolic volume = 50mL
o Stroke volume = 80mL
o Ejection fraction = 65%
• Cardiac function curve
o Increasing venous return increases the ventricular end diastolic
volume and stretches the
ventricles
o Stretching the muscle cell
increases the pressure they can
generate
o Increasing pressure increases
stroke volume
o Frank Starling Law → within
physiological limits the heart
pumps all the blood it receives
o Increased venous return
stretches the ventricles and
increases force production
until cardiac output matches
venous return → heart stops
expanding
Flow:
• Flow requires a pressure difference
• Blood flows from high to low pressure
• Transmule pressure → pressure difference between the inside and
outside of a vessel
• Flow through the vascular system is produced by the arterial to venous
blood pressure
• Flow is the same through regions connected in series
• Flow in = flow out
• Volume cannot change
find more resources at oneclass.com
find more resources at oneclass.com

• If volumes are changing, cardiac output and venous return will be
different
• Volumes change due to constriction/dilation of veins
Electrical Conductivity of the Heart:
• Within atria and ventricles myocardial cells are connected by gap
junctions
• Gap junctions allow the cardiac action potential to propagate from cell to
cell through a low resistance pathway
• Heart has its own pacemaker → no hormones needed
• Electrical activity can pass from cell to cell in the atria and ventricles
• Atria and ventricles are electrically isolated by annulus fibrosis
• Heart has specialized electrically active cells in addition to contractile
myocardium, which form the
o SA node
o AV node
o Bundle of HIS
o Purkinje fibers
o These cells show autorhythmicity → ability to generate a heart
beat → does not require nerve or horomonal input to beat
▪ SA node → fastest pacemaker potential → 90-100
beats/min
▪ AV node → second pacemaker → 40-60 beats/min
▪ Bundle of HIS → last pacemaker → 15-30 beats/min
• Electrical activity normally originates in the SA node → drives the heart
and suppresses other pacemakers
• The AV node forms the only site of electrical connection between the atria
and ventricles
• Propagation of the cardiac action potential
o Starts in the SA node
o AP conducted through atrial muscle
o AP is delayed at AV node before entering the Bundle of HIS → lets
atria contract
o Conduction through the Bundle of HIS and Purkinje fibers is very
rapid
o Ventricles depolarize from endo to epicardium and from apex to
base
o Ectopic beats → beats generated outside the normal pacemaker
• Neural control of the heart
o At rest the heart is under parasympathetic tone → slows natural
rhythm of heart
o Agents that alter heart rate are chronotropic
▪ Positive chronotropic agents
• Increase heart rate
• E.g. adrenaline and noradrenaline acting on -
adrenergic receptors on the heart
▪ Negative chronotropic agents
• Slow the heart
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
120/80: pulse pressure 40mmhg difference between systolic and diastolic pressure. If volumes are changing, cardiac output and venous return will be different: volumes change due to constriction/dilation of veins. Increase heart rate: e. g. adrenaline and noradrenaline acting on (cid:2010)- adrenergic receptors on the heart, negative chronotropic agents, slow the heart, e. g. acetylcholine acting on m-cholinergic receptors on the heart. Mean arterial pressure: map = cardiac output x total resistance, sets systolic and diastolic pressures. Increase in cardiac output = increase in map. Increase heart rate/stroke volume = increase cardiac output = increase. Microcirculation: consists of, arterioles, venules, metarterioles, capillaries, atriovenous shunts, transport across the capillary wall, transport can be, paracellular or transcellular, active or passive, bulk flow or diffusion, lipid soluble substances pass through the cell membranes o2 or. Increased filtration oedema: vasodilation increase capillary blood pressure, arterial and venous hypertension increase capillary blood pressure, increased plasma leakage most common, lose osmotic pressure, plasma protein deficiency.