PSY353 Chapter Notes - Chapter 12: Cluster B Personality Disorders, Antisocial Personality Disorder, Personality Disorder


CHAPTER 12: Personality Disorders
AN OVERVIEW OF PERSONALITY DISORDERS
We all think we know what a personality is
• It’s all the haateisti ays a person behaves and thinks
• We tend to type people as behaving in one way in many situations
• We also have all probably behaved in all the other ways noted here (dramatic, suspicious, outgoing, easily upset).
Personality disorders – when personality characteristics interfere with relationships with others, cause the person distress, or in general
disrupt activities of daily living
ASPECTS OF PERSONALITY DISORDERS
Personality disorders are chronic → unlike other disorders
• they do not come and go
• originate in childhood and continue throughout adulthood
• these chronic problems affect personality
• pervade eve aspet of a peso’s life
Personality disorder – a persistent pattern of emotions, cognitions, and behavior that results in enduring emotional distress for the person
affected and/or for others and may cause difficulties with work and relationships
• DSM-5 lists 10 specific personality disorders
• DSM-5 notes that having a personality disorder may distress the affected person
• BUT individuals with personality disorders may not feel any subjective distress
• may in fact be others who acutely feel distress because of the actions of the person with the disorder
• particularly common with antisocial personality disorder → individual may show a blatant disregard for the rights of others yet
exhibit no remorse
• someone other than the person with the personality disorder must decide whether the disorder is causing significant functional
impairment → affected person often cannot make such a judgment
Prospects for treatment success for people who have personality disorders may be more optimistic than previously thought
• but many people who have personality disorders in addition to other psychological problems tend to do poorly in treatment
How the therapist feels about the client → affects treatment outcome
• countertransference – emotions of therapists brought out by clients → tend to be negative for those diagnosed with personality
disorders, especially those in Cluster A (the odd or eccentric cluster) and Cluster B (the dramatic, emotional, or erratic cluster)
• therapists especially need to guard against letting their personal feelings interfere with treatment when working with people who
have personality disorders
Prior to DSM-5 → most disorders were in Axis I of the DSM-IV-TR → included the traditional disorders
• personality disorders were included in a separate axis (Axis II) → seen as distinct as a group
• characteristic traits were more ingrained and inflexible in people who have personality disorders
• disorders themselves were less likely to be successfully modified
• separate axes were eliminated in DSM-5 → personality disorders are listed with the rest of the DSM-5 disorders
Category of personality disorders is controversial → it involves a number of unresolved issues
CATEGORICAL AND DIMENSIONAL MODELS
People with personality disorders display problem characteristics over extended periods and in many situations
• can cause great emotional pain for themselves, others, or both
• their difficulty, then, can be seen as one of degree rather than kind
• problems of people with personality disorders may just be extreme versions of the problems many of us experience temporarily →
as being shy or suspicious
Distinction between problems of degree and problems of kind → usually described in terms of dimensions instead of categories
find more resources at oneclass.com
find more resources at oneclass.com

Debate: whether personality disorders are extreme versions of otherwise typical personality variations (dimensions) or ways of relating that
are different from psychologically healthy behavior (categories)
• we tend to look at gender categorically → male or female
• many believe it is more accurate to look at gender in terms of dimensions → place people along a continuum of maleness and
femaleness rather than in the absolute categories of male or female
Many researchers and clinicians see personality disorders as extremes on one or more personality dimensions
• because of the way people are diagnosed with the DSM → personality disorders end up being viewed in categories
• either you do or you do not have a disorder
• DSM diagnoses do’t ate ho depedet ou ae → if you meet the criteria, you are labeled as having dependent personality
disorder
• thee is o soehat he it oes to personality disorders
There are advantages to using categorical models of behavior → most important being their convenience
• But simplification have problems → the mere act of using categories leads clinicians to reify them → to view disorders as real
thigs, comparable to the realness of an infection or a broken arm
• Some argue that personality disorders are not things that exist but points at which society decides a particular way of relating to the
world has become a problem
Some had proposed that the DSM-5 personality disorders section be replaced or at least supplemented by a dimensional model
• individuals would not only be given categorical diagnoses but also would be rated on a series of personality dimensions.
• such a system would have at least three advantages over a purely categorical system:
1. it would retain more information about each individual
2. it would be more flexible because it would permit both categorical and dimensional differentiations among individuals
3. it would avoid the often arbitrary decisions involved in assigning a person to a diagnostic category
Alternative model of personality disorders → iluded i the setio o eegig easues ad odels in DSM-5
• model focuses on a continuu of distuaes of self (i.e., how you view yourself and your ability to be self-directed) and
interpersonal (i.e., your ability to empathize and be intimate with others) functioning
• remains to be seen how this alternative model will be used in the future
No general consensus exists about what the basic personality dimensions might be → several contenders
The five-factor model Big Fie) – taken from work on normal personality
• people can be rated on a series of personality dimensions
• on each dimension, people are rated high, low, or somewhere between
• the combination of five components describes why people are so different
• factors or dimensions include:
1. extroversion: talkative, assertive, and active | silent, passive, and reserved
2. agreeableness: kind, trusting, and warm | hostile, selfish, and mistrustful
3. conscientiousness: organized, thorough, and reliable | careless, negligent, and unreliable
4. neuroticism: even-tempered | nervous, moody, and temperamental
5. openness to experience: imaginative, curious, and creative | shallow and imperceptive
Cross-cultural research establishes the relatively universal nature of the five dimensions → BUT there are individual differences across cultures
Big Five traits in high school students across 6 different cultures and found
• Turkey → higher levels of conscientiousness and extraversion than those in China
• Taiwan → as much openness as those in Slovenia
A number of researchers are trying to determine whether:
• people with personality disorders can also be rated in a meaningful way along the Big Five dimensions
• the system will help us better understand these disorders
find more resources at oneclass.com
find more resources at oneclass.com

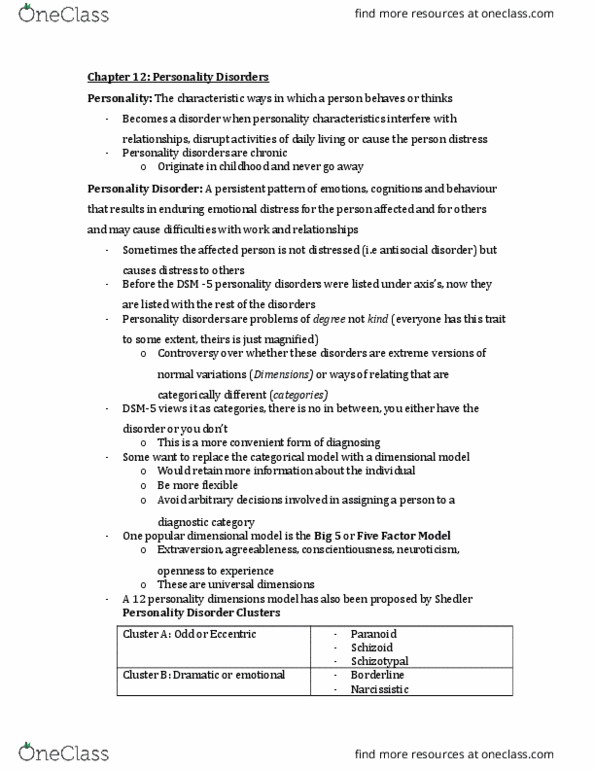
PERSONALITY DISORDER CLUSTERS
DSM-5 divides the personality disorders into 3 groups, or clusters
• will probably continue until a strong scientific basis is established for viewing them differently
• cluster division is based on resemblance
PERSONALITY DISORDER CLUSTERS
Cluster A – odd or eccentric disorders
Paranoid personality disorder
A pervasive distrust and suspiciousness of others such
that their motives are interpreted as malevolent.
I cannot trust people.
Schizoid personality disorder
A pervasive pattern of detachment from social
relationships and a restricted range of expression of
emotions in interpersonal settings.
It’s ette to e isolated fo othes.
Schizotypal personality disorder
A pervasive pattern of social and interpersonal deficits
marked by acute discomfort with reduced capacity for
close relationships, as well as by cognitive or
perceptual distortions and eccentricities of behaviour.
Relationships are messy, undesirable.
Cluster B – dramatic, emotional, or erratic disorders
Antisocial personality disorder
A pervasive pattern of disregard for and violation of
the rights of others.
I am entitled to break rules.
Borderline personality disorder
A pervasive pattern of instability of interpersonal
relationships, self-image, affects, and control over
impulses.
I deserve to be punished.
Histrionic personality disorder
A pervasive pattern of excessive emotion and
attention seeking.
People are there to serve or admire me.
Narcissistic personality disorder
A pervasive pattern of grandiosity (in fantasy or
behaviour), need for admiration, and lack of empathy.
Since I am special, I deserve special rules.
Cluster C – anxious or fearful disorders
Avoidant personality disorder
A pervasive pattern of social inhibition, feelings of
inadequacy, and hypersensitivity to negative
evaluation.
If people ke the eal e, the ould
reject me.
Dependent personality disorder
A pervasive and excess need to be taken care of, which
leads to submissive and clinging behaviour and fears of
separation.
I need people to survive, be happy.
Obsessive-compulsive personality
disorder
A pervasive pattern of preoccupation with orderliness,
perfectionism, and mental and interpersonal control,
at the expense of flexibility, openness, and efficiency.
People should do better, try harder.
STATISTICS AND DEVELOPMENT
Many people with these problems do not seek help on their own as do those with many of the other DSM-5 disorders
• gathering information about the prevalence of personality disorders is difficult → varies a great deal
• 1 in 10 adults in the US may have a diagnosable personality disorder → makes them relatively common
• numbers vary somewhat across countries
• 6% of adults may have at least one personality disorder worldwide
• differences in prevalence estimates → result of different survey methods: surveying people in clinical settings versus surveying the
general population (even those not seeking assistance)
• gender differences → highly variable when surveying the general population
Reasons for these differences in diagnoses:
- bias in diagnoses
- differences in help-seeking behavior
- tolerance of behavior in a culture
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
We all think we know what a personality is. Personality disorders when personality characteristics interfere with relationships with others, cause the person distress, or in general disrupt activities of daily living. Personality disorders are chronic unlike other disorders they do not come and go originate in childhood and continue throughout adulthood these chronic problems affect personality pervade eve(cid:396)(cid:455) aspe(cid:272)t of a pe(cid:396)so(cid:374)"s life. Personality disorder a persistent pattern of emotions, cognitions, and behavior that results in enduring emotional distress for the person affected and/or for others and may cause difficulties with work and relationships. Dsm-5 notes that having a personality disorder may distress the affected person. Prospects for treatment success for people who have personality disorders may be more optimistic than previously thought but many people who have personality disorders in addition to other psychological problems tend to do poorly in treatment. Category of personality disorders is controversial it involves a number of unresolved issues.