BIOLOGY 2F03 Chapter Notes - Chapter 9-11: Erythrocyte Fragility, Hereditary Spherocytosis, Glucose-6-Phosphate Dehydrogenase Deficiency

20 May 2018
School
Department
Course
Professor

Suspicion of inherited HA from history
• Young age/ congenital
• Episodic haemolysis may point more to something like G6PD
• Mode of inheritance/ family Hx
• Other systemic disorders (eg neuro/ myopathy trouble with enzyme deficiencies without multiple
isoforms)
Lab features of inherited HA
• Film - Anaemia, reticulocytosis, polychromasia
• Bloods - high BR, LDH & low (used up) haptoglobins in intravascular haemolysis
• Urine - haemoglobinuria (red)/ haemosiderinuria (brown) in intravascular haemolysis
1. Red cell membrane disorders
Red cell cytoskeletal proteins are numbered in the order they separate on electrophoresis
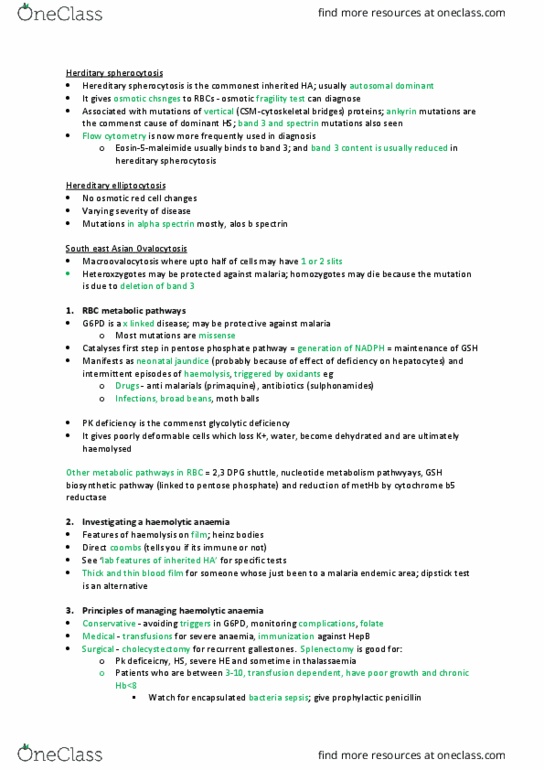
Herditary spherocytosis
• Hereditary spherocytosis is the commonest inherited HA; usually autosomal dominant
• It gives osmotic chsnges to RBCs - osmotic fragility test can diagnose
• Associated with mutations of vertical (CSM-cytoskeletal bridges) proteins; ankyrin mutations are the
commenst cause of dominant HS; band 3 and spectrin mutations also seen
• Flow cytometry is now more frequently used in diagnosis
o Eosin-5-maleimide usually binds to band 3; and band 3 content is usually reduced in
hereditary spherocytosis
Hereditary elliptocytosis
• No osmotic red cell changes
• Varying severity of disease
• Mutations in alpha spectrin mostly, alos b spectrin
South east Asian Ovalocytosis
• Macroovalocytosis where upto half of cells may have 1 or 2 slits
• Heteroxzygotes may be protected against malaria; homozygotes may die because the mutation is
due to deletion of band 3
2. RBC metabolic pathways
• G6PD is a x linked disease; may be protective against malaria
o Most mutations are missense
• Catalyses first step in pentose phosphate pathway = generation of NADPH = maintenance of GSH
• Manifests as neonatal jaundice (probably because of effect of deficiency on hepatocytes) and
intermittent episodes of haemolysis, triggered by oxidants eg
o Drugs - anti malarials (primaquine), antibiotics (sulphonamides)
o Infections, broad beans, moth balls
• PK deficiency is the commenst glycolytic deficiency
• It gives poorly deformable cells which loss K+, water, become dehydrated and are ultimately
haemolysed
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Suspicion of inherited ha from history: young age/ congenital, episodic haemolysis may point more to something like g6pd, mode of inheritance/ family hx, other systemic disorders (eg neuro/ myopathy trouble with enzyme deficiencies without multiple isoforms) Lab features of inherited ha: film - anaemia, reticulocytosis, polychromasia, bloods - high br, ldh & low (used up) haptoglobins in intravascular haemolysis, urine - haemoglobinuria (red)/ haemosiderinuria (brown) in intravascular haemolysis, red cell membrane disorders. Red cell cytoskeletal proteins are numbered in the order they separate on electrophoresis. Herditary spherocytosis: hereditary spherocytosis is the commonest inherited ha; usually autosomal dominant, associated with mutations of vertical (csm-cytoskeletal bridges) proteins; ankyrin mutations are the. Hereditary elliptocytosis: no osmotic red cell changes, varying severity of disease, mutations in alpha spectrin mostly, alos b spectrin. Infections, broad beans, moth balls: pk deficiency is the commenst glycolytic deficiency. It gives poorly deformable cells which loss k+, water, become dehydrated and are ultimately haemolysed.