KINESIOL 1Y03 Chapter Notes - Chapter 12: Cholangiocyte, Cirrhosis, Cholecystitis

22 Jun 2018
School
Department
Course
Professor

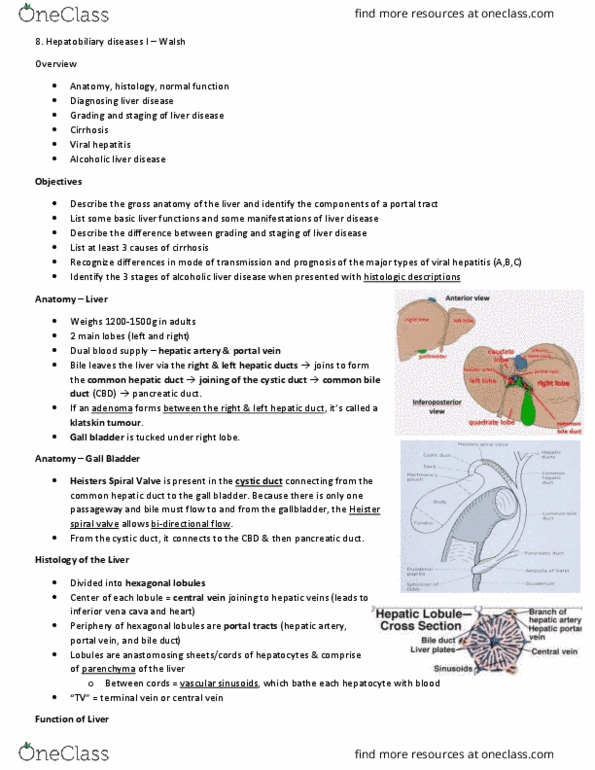
Bile duct tumours
Bile duct adenomas
Benign, incidental tumours
Small white nodule composed of proliferating bile ducts
Cholangiocarcinoma
Seen both inside and outside the liver, all the way through to the gallbladder and
common bile duct
95% are well-differentiated adenocarcinomas i.e. form glands and produce mucin
this means they can be confused with metastases from other tumours metastasizing to
the liver
they have marked fibrosis i.e. are desmoplastic, with lots of stroma (c.f. HCC rare
tumour which doesn’t have fibrosis)
may see dysplasia locally (this confirms it is a primary as it is local evidence of
progression)
Can also be adenosquamous etc (see slides)
Haaematogenous and lymphatic spread relatively common
Prognosis very poor worldwide (may be better with aggressive chemotherapy and
skilled hepato-biliary surgeons)
Classification of location
1) peripheral
2) a + b: right and left hepatic ducts
3) confluence / hilar / Klatskin tumours
4) common hepatic duct
5) gallbladder
6) cystic duct
7) common bile duct
whether a tumour is classified as intrahepatic or extrahepatic determines epidemiological
classfication
ICC can be mass-forming, peri-ductal infiltrative, intraductal growing
ECC can be nodular, sclerosing, or papillary
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Small white nodule composed of proliferating bile ducts. Seen both inside and outside the liver, all the way through to the gallbladder and common bile duct. 95% are well-differentiated adenocarcinomas i. e. form glands and produce mucin this means they can be confused with metastases from other tumours metastasizing to the liver they have marked fibrosis i. e. are desmoplastic, with lots of stroma (c. f. Hcc rare tumour which doesn"t have fibrosis) May see dysplasia locally (this confirms it is a primary as it is local evidence of progression) Prognosis very poor worldwide (may be better with aggressive chemotherapy and skilled hepato-biliary surgeons) Classification of location: peripheral, a + b: right and left hepatic ducts, confluence / hilar / klatskin tumours, common hepatic duct, gallbladder, cystic duct, common bile duct. Whether a tumour is classified as intrahepatic or extrahepatic determines epidemiological classfication. Icc can be mass-forming, peri-ductal infiltrative, intraductal growing. Ecc can be nodular, sclerosing, or papillary.