PHTY102 Lecture Notes - Lecture 10: Spasm, Ulnar Nerve, Edema


10. Principles of passive movement
• Define the term passive movements
o Movement of a joint or body segment by a force external to the body, without
active, voluntary muscle contraction by the individual
• Differentiate between passive movements and other types of joint movement
o Passive
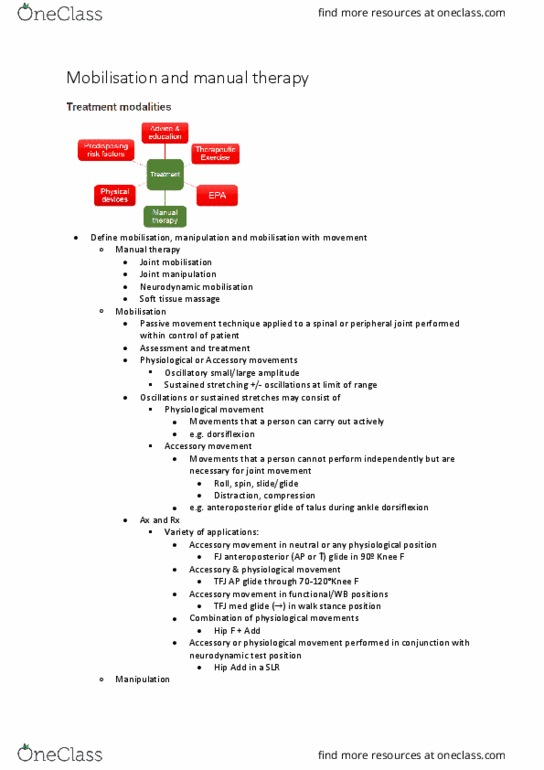
• Terminology associated with passive joint movement - mobilisation and
manipulation
▪ Manipulation Specialised technique performed through a few degrees
of motion at the end of joint range
▪ Forceful high velocity thrust in localised area - most commonly spine
• Passive physiological
▪ Performed through normal physiological range of movement present in
joint
▪ e.g. shoulder flexion, hip extension, thumb abduction, neck rotation
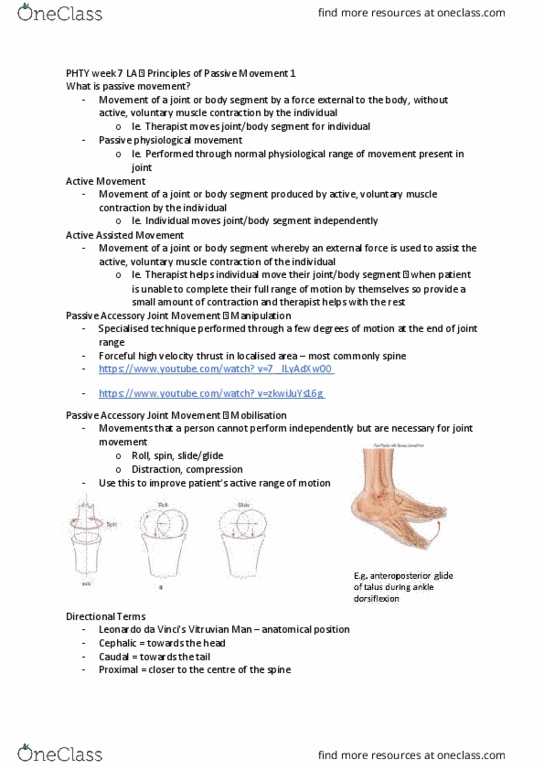
• Passive accessory - mobilisation
▪ Movements that a person cannot perform independently but are
necessary for joint movement
▪ Can take the joint further than normal
▪ Roll, spin, slide/glide
▪ Distraction, compressions
▪ e.g. anteroposterior glide of talus during ankle dorsiflexion
o Active
find more resources at oneclass.com
find more resources at oneclass.com

• Movement of a joint or body segment produced by active, voluntary muscle
contraction by the individual
• Individual moves joint/body segment independently
o Active assisted
• Movement of a joint or body segment whereby an external force is used to
assist the active, voluntary muscle contraction of the individual
• Describe the anatomical planes of joint movement
Frontal/coronal - vertical plane that divides the body into front and back
find more resources at oneclass.com
find more resources at oneclass.com

• Joint movement
▪ Abduction and adduction
▪ Ankle inversion and eversion
▪ Ulnar and radial deviation
Sagittal - vertical plane that divides the body into right and left sides
• Joint movement
▪ Flexion and extension
Transverse - horizontal plane that divides the body into upper and lower
components
• Joint movement
▪ Rotation
▪ Scapula adduction/retraction and abduction/protraction
o Range of movement
• The amount of movement that occurs at a joint
• The amount of motion possible between two bony levers
• Identify and describe the indications for use of passive movements in physiotherapy
practice
o Indications
• To become familiar with joint movement
• To assess an individual's range of movement when other factors may be
preventing active full range
▪ e.g. weakness, tendon pathology, pain, semi/unconscious, paralysis,
poor motor coordination
• Passive movements can be used to gain information about joint integrity,
muscle tone (velocity dependent passive movement), reflexes
• Passive movement cannot:
▪ Prevent muscle atrophy
▪ Increase muscle strength or endurance
▪ Reduce adipose tissue
o Levels of evidence for use
• Counteract negative effects of immobilisation
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Individual moves joint/body segment independently: active assisted, movement of a joint or body segment whereby an external force is used to assist the active, voluntary muscle contraction of the individual, describe the anatomical planes of joint movement. Frontal/coronal - vertical plane that divides the body into front and back. Joint movement: abduction and adduction, ankle inversion and eversion, ulnar and radial deviation. Sagittal - vertical plane that divides the body into right and left sides. Transverse - horizontal plane that divides the body into upper and lower components. Scapula adduction/retraction and abduction/protraction: range of movement, the amount of movement that occurs at a joint, the amount of motion possible between two bony levers. Identify and describe the indications for use of passive movements in physiotherapy practice. Support and stability of the trunk and extremities: patient comfort (and therapist comfort/safety, neutral position of limbs not being moved, provide access and exposure to areas to be moved, draping.