PSYC10003 Lecture Notes - Lecture 9: Primary Motor Cortex, Premotor Cortex, Motor Neuron

12 Jun 2018
School
Department
Course
Professor

Lecture 9, Monday 21 March 2016
PSYC10003 - MIND, BRAIN & BEHAVIOUR 1
LECTURE 9
THE SENSORIMOTOR SYSTEM
TWO PATIENTS WITH MOTOR IMPAIRMENTS AFTER
STROKE
•It is not until something goes wrong with the system that lets us
walk and move automatically that we realise how important
movement is for everyday behaviour.
•Let us consider two patients seen by a clinical neuropsychologist,
both of whom had profound losses of motor control (i.e., the
control of body movement) for limbs on the left side of their body.
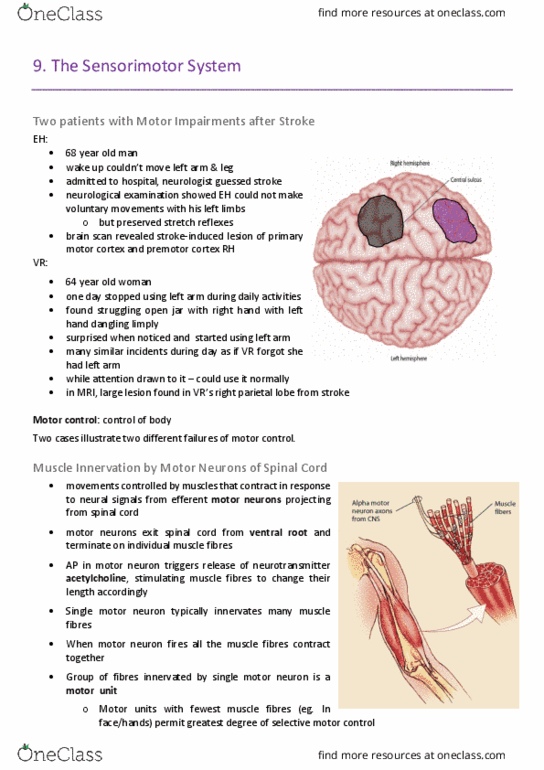
•Patient EH is a 68 year old man who awoke one morning to find
he could not move his left arm or leg. He was admitted to hospital,
at which time the examining neurologist guessed that EH had
suffered a stroke. The neurological examination showed that even
though EH could not make voluntary movements with his left
limbs, he had preserved stretch reflexes (in fact his reflexes on the
left were even stronger than those on the right). An MRI scan of
EH’s brain revealed a stroke-induced lesion of the primary motor
cortex and premotor cortex of the right hemisphere.
•Patient VR is a 64 year old woman who one day stopped using her
left arm during her daily activities. Her daughter found her struggling to open a jar with her right
hand, and noticed that her left hand was dangling limply by her side. When she suggested to VR
that she hold the jar steady with her left hand, her mother looked down by her side with a
surprised look, raised her left hand, grabbed the jar and promptly twisted the lid off. During the
day there were many similar incidents. It was as if VR had forgotten that she had a left arm at all,
even though when her attention was drawn to it she seemed able to use it normally. Frightened by
these strange symptoms, VR’s daughter took her mother to hospital. After undergoing an MRI
scan, a large lesion was found in VR’s right parietal lobe, the result of a recent stroke.
•These two cases illustrate two different failures of motor control. To understand the basis for
these failures, we need to consider which parts of the human CNS are involved in sensorimotor
control, and how these areas perform the complex processes involved in motor control.
MUSCLE INNERVATION BY MOTOR NEURONS OF SPINAL CORD
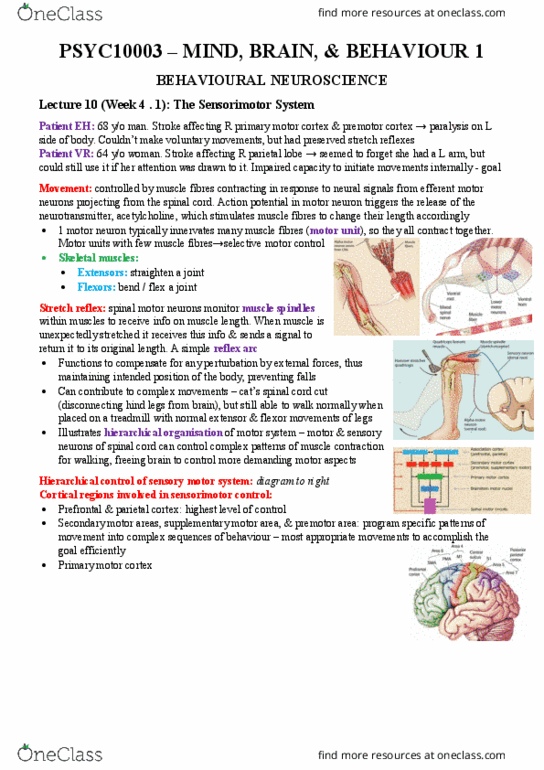
•Movements are controlled by muscles that contract in response to neural signals from efferent
motor neurons projecting from the spinal cord. Motor neurons exit the spinal cord via the ventral
root and terminate on individual muscle fibres.
•An action potential in a motor neuron triggers the release of a neurotransmitter, acetylcholine,
which stimulates muscle
fibres to change their length
accordingly.
•A single motor neuron
typically innervates many
muscle fibres; when the
motor neuron fires all the
muscle fibres contract
together.
•The group of fibres
innervated by a single motor
neuron is called a motor
unit. Motor units with the

Lecture 9, Monday 21 March 2016
PSYC10003 - MIND, BRAIN & BEHAVIOUR 1
•fewest muscle fibres, such as those in the face and hands, permit the greatest degree of selective
motor control.
•Many skeletal muscles fall into one of two categories: extensors and flexors.
‣Flexors act to bend or ‘flex’ a joint, whereas extensors act to straighten it.
‣These two categories of muscle often act antagonistically (i.e., in opposition), as is the case for
the biceps and triceps muscles in the
upper arm.
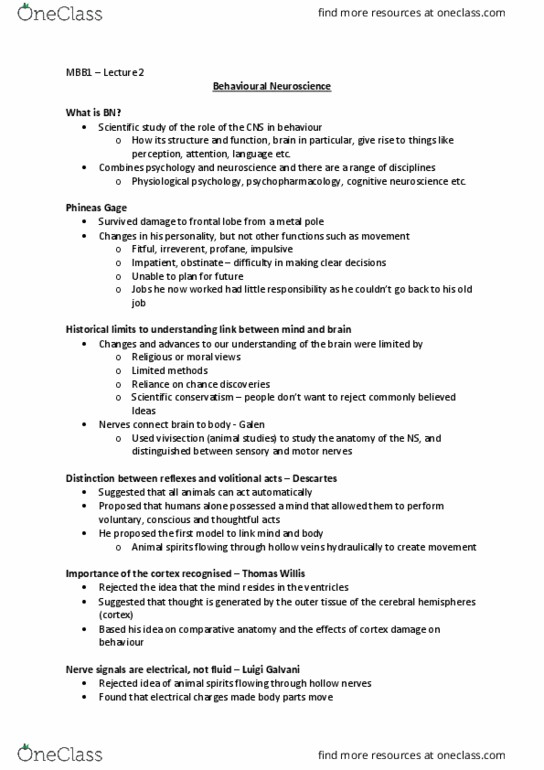
STRETCH REFLEX
•Spinal motor neurons receive input
from a variety of sources. One such
source is the sensory receptors located
within the muscles themselves.
•The activity of skeletal muscles is
monitored by receptors called muscle
spindles, which provide information to
the CNS regarding muscle length.
•When a muscle is unexpectedly
stretched, as occurs when a hammer is
used to tap beneath the patella
(kneecap), the muscle spindles convey
information back to the spinal cord via the dorsal roots.
•The axons of spindle afferent neurons synapse directly with the motor neurons, which increase
their activity in order to return the muscle to its original length.
‣This results in a brisk contraction of the quadriceps muscle, which causes the lower leg to
extend. This circuit forms a simple reflex arc. (movement without brain involvement)
•When a doctor elicits the patellar tendon reflex just described, the effects are readily noticeable,
but the functional significance of the reflex is more subtle.
•The role of such simple stretch reflexes is to compensate for any perturbation by external forces
and thus maintain the intended position of the body. Thus, for example, when someone bumps
into you from behind or brushes your arm while you’re carrying a hot cup of coffee, the stretch
reflex compensates automatically and prevents you from falling over or spilling your drink.
•The patients EH and VR both had strong patellar tendon reflexes, indicating that the motor and
sensory neurons of the spinal cord remained intact.
•The point of this stretch reflex is that it enables people to assess the functioning of their motor
pathway at its lowest levels.
PRESERVED WALKING FOLLOWING SPINAL CORD RESECTION
•Motor neurons in the spinal cord are capable of triggering quite complex movements of various
muscle groups, without any controlling signals from the brain. This has been illustrated in
experiments with cats, in which the spinal cord is surgically sectioned at a point just above where
the spinal nerves subserving the hind legs are located. This effectively disconnects the lower motor
neurons for the hind legs from
the brain.
•Despite this spinal cord section,
the cats are still able to walk
normally when placed on a
treadmill, showing normal
extensor and flexor movements
of the hind legs.
•This is a dramatic illustration of
the hierarchical organisation of
the motor system.

Lecture 9, Monday 21 March 2016
PSYC10003 - MIND, BRAIN & BEHAVIOUR 1
•Motor and sensory neurons within the spinal cord are able to control all of the complex patterns
of muscle contraction required for walking, without any instructions from the brain.
•This leaves the brain free to control the more demanding aspects of motor control, such as
determining precisely when to initiate particular actions, which effectors to use, and how to tailor
movements to the specific environment in which the organism finds itself.
DESCENDING CONTROL FROM THE BRAIN
•Most purposeful actions are initiated and controlled voluntarily, and such actions depend upon
signals generated by the brain that are conveyed to the muscles via the spinal cord.
•Reflexes can be modulated by control signals from the brain.
•In the example of carrying a hot casserole dish, the tendency to want to drop the dish comes from
excitatory synapses on motor neurons in the spinal cord. But this excitation can be counteracted
by inhibitory input from the
primary motor cortex in the
brain.
•The axons that descend from
the primary motor cortex
through the spinal cord form
inhibitory synapses with lower
motor neurons. These
inhibitory synapses can
prevent a muscle contraction
from occurring by blocking
action potentials in lower
motor neurons.
•Similarly, excitatory inputs
from the brain can trigger
action potentials in lower
motor neurons and initiate
movements.
•The stroke patient EH, whose
right primary motor cortex
and premotor cortex are
damaged, is unable to make
voluntary movements with his
left arm and leg, suggesting that signals from the primary motor cortex are evidently needed for
voluntary movement of the contralateral limbs.
•Patient VR, by contrast, is able to make normal limb movements when prompted, but fails to do
so spontaneously. Her parietal lesion therefore seems to have affected her capacity to initiate
movements internally.
HIERARCHICAL CONTROL IN THE SENSORIMOTOR SYSTEM
•The human sensorimotor system can be thought of as somewhat analogous to a large and
efficient company, in which commands are issued in a top-down manner.
•The association areas (prefrontal cortex and parietal cortex) act as the president or general
manager, specifying general goals rather
than specific plans of action.
‣Just like a general manager, the
association cortex is not routinely
involved in the details. This leaves the
highest levels of control free to
perform the most complex functions.
Document Summary
He was admitted to hospital, at which time the examining neurologist guessed that eh had suffered a stroke. The neurological examination showed that even though eh could not make voluntary movements with his left limbs, he had preserved stretch reflexes (in fact his reflexes on the left were even stronger than those on the right). Eh"s brain revealed a stroke-induced lesion of the primary motor cortex and premotor cortex of the right hemisphere: patient vr is a 64 year old woman who one day stopped using her left arm during her daily activities. Her daughter found her struggling to open a jar with her right hand, and noticed that her left hand was dangling limply by her side. When she suggested to vr that she hold the jar steady with her left hand, her mother looked down by her side with a surprised look, raised her left hand, grabbed the jar and promptly twisted the lid off.