PSYC30014 Lecture Notes - Lecture 10: Somatic Symptom Disorder, Dissociative Identity Disorder, Medically Unexplained Physical Symptoms

18 Jun 2018
School
Department
Course
Professor

Lecture 10
- Lecture objectives:
- •To outline the clinical pictures of the various disorders within these sections of
DSM5 - similarities and differences
- •To outline the putative predisposing and precipitating aetiological factors and
maintaining factors of some of these disorders
- •To raise questions about these ‘disorders’ and outline some controversial issues
- Somatic Symptom Disorders [about the body]:
- ‘All of the disorders in this chapter share a common feature: the prominence of ➱
somatic symptoms [aren’t medically explained; concerns or responses to bodily
symptoms that are along the lines of profound psychological distress,
disproportionate concern, worry and so forth] associated with significant distress and
impairment.’ (source: DSM5)
- ‘Mental disorders that take the form of physical disorders’ (Clarke & Gleaves, in ➱
Rieger)
- (Somatic symptoms = physical symptoms)➱
- Expression of psychological distress through physiological symptomatology
- Dissociative disorders are characterised by a disruption of and/or discontinuity
[fracturing in higher order mental processes] in the normal integration of
consciousness, memory, identity, emotion, perception, body representation, motor
control, and behaviour. Dissociative symptoms can potentially disrupt every area of
psychological functioning. (Source: DSM5)
- Multiple Personality Disorder is now called Dissociative Identity Disorder
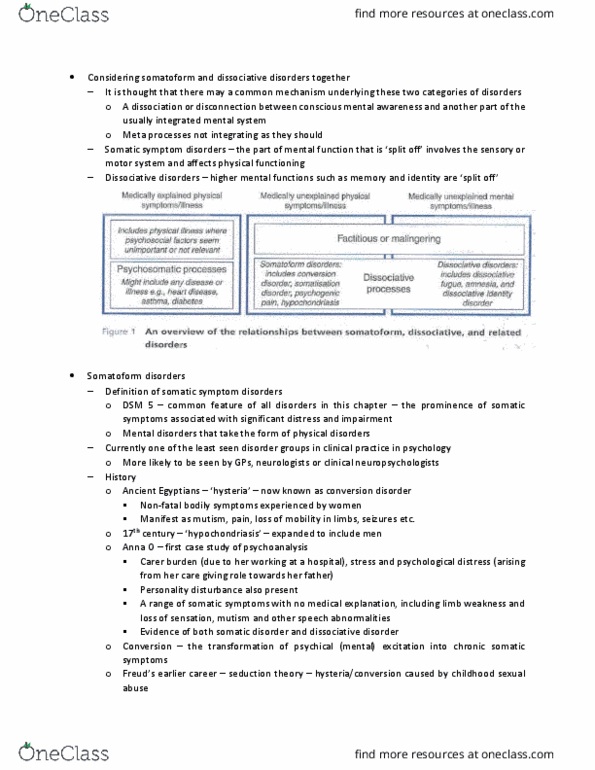
- It is thought that there may be a common mechanism underlying these disorders -
specifically, a dissociation or disconnect [fracturing in mental system at some level]
between conscious mental awareness and another part of the usually integrated
mental system
- → Somatic symptom disorders - the part of mental function that is ‘split off’ involves
the sensory or motor system and affects physical functioning [fracturing of conscious
processes and motor and sensory processes; relatively low level experiences in
terms of hierarchy of psychological functioning];
- → Dissociative disorders - higher mental functions such as memory or identity are
‘split off’ [experience of self and world phenomenologically, personality and
experience of emotions]
find more resources at oneclass.com
find more resources at oneclass.com

-
- Common thread: fracturing/dissociative process in terms of mental processes not
integrating as they should
- The experience of encountering a medically unexplained symptom is not necessarily
pathological - happen to most of population to more or less degree
- Implications around mood (e.g. depressed, get one down, become anxious);
behaviour (in terms of cognition, thoughts - ruminate on problem, engage in help-
seeking behaviour)
- Would issue get worse over time when engage in it along this line?
- What sort of experiences might maintain or make symptom worse?
- Currently one of the least seen disorder groups in clinical practice in psychology.
More likely to be seen by GPs, neurologists or clinical neuropsychologists
- Long history of thinking about this phenomena - many theoretical approaches
- Ancient Egyptians (Kahun Medical Papyrus - 1900BC) and Hippocrates (500BC) -
‘hysteria’ - non-fatal bodily symptoms experienced by women (wandering uterus)
- 17th century - ‘hypochondriasis’ - males too
- • Anna O - first case study of psychoanalysis (Freud & Breuer, 1893).
- → Carer burden, stress, and psychological distress
- → A range of somatic symptoms with no medical explanation, including limb
weakness and loss of sensation, mutism and other speech abnormalities.
- → Also personality disturbance.
- • Conversion - ‘transformation of psychical [mental] excitation into chronic somatic
symptoms’ [conversion of psychological distress into physiological
expressions/somatic symptoms]
find more resources at oneclass.com
find more resources at oneclass.com

- • Freud’s earlier career – hysteria/conversion caused by childhood sexual abuse –
‘seduction theory’ [childhood sexual abuse and trauma is a precursor to conversion
disorder]. Perhaps recanted under pressure. Now holds more weight.
-
- Somatisation: underlies all of the somatic symptom disorders; distress is experienced
as physical symptoms [or in response to physiological symptoms] or altered bodily
function; not necessarily ‘abnormal’ - despite DSM assuming a clear demarcation
between normal and abnormal
- Sometimes difficult to distinguish between physical disorder and somatoform disorder
- → How many physical symptoms are being described and for how long? [greater
number → higher chances of somatoform disorder]
- → What degree of bodily preoccupation is there? [more → higher chances]
- → How intensely does the individual worry about their health and illness? [potential
developing illness or about already having the illness]
- → How forcefully do they seek healthcare? [believe doctors or not be convinced and
do more tests]
- → Is there a history of disgruntlement with the healthcare system? [doctor shopping -
go to a doctor → don’t get answer they want → go to another doctor; or get answer
they want and not be reassured or feel like they know better]
- Sometimes difficult to distinguish these disorders from other psychological
conditions:
- ⇒Heart palpitations and upset stomach- not uncommon in relation to anxiety;
- Fatigue- ⇒not uncommon in depression
- ⇒Vomiting and weight change- not uncommon in eating disorders
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Lecture objectives: to outline the clinical pictures of the various disorders within these sections of. Dsm5 - similarities and differences: to outline the putative predisposing and precipitating aetiological factors and maintaining factors of some of these disorders, to raise questions about these disorders" and outline some controversial issues. Mental disorders that take the form of physical disorders" (clarke & gleaves, in. Expression of psychological distress through physiological symptomatology. Dissociative disorders are characterised by a disruption of and/or discontinuity. [fracturing in higher order mental processes] in the normal integration of consciousness, memory, identity, emotion, perception, body representation, motor control, and behaviour. Dissociative symptoms can potentially disrupt every area of psychological functioning. (source: dsm5) Multiple personality disorder is now called dissociative identity disorder. It is thought that there may be a common mechanism underlying these disorders - specifically, a dissociation or disconnect [fracturing in mental system at some level] between conscious mental awareness and another part of the usually integrated mental system.