CAM201 Lecture Notes - Lecture 8: European Cooperation In Science And Technology, Inotrope, Vasodilation


Learning Objectives
• Understand and identify key features of the PV loop
• Describe how preload, afterload and contractility interact with each other
• Define and explain the differences between systolic and diastolic HF
• Understand how myocardial function changes in HF and the adaptive changes that follow
• Understand the adaptations in chronic volume and pressure overload leading to HF
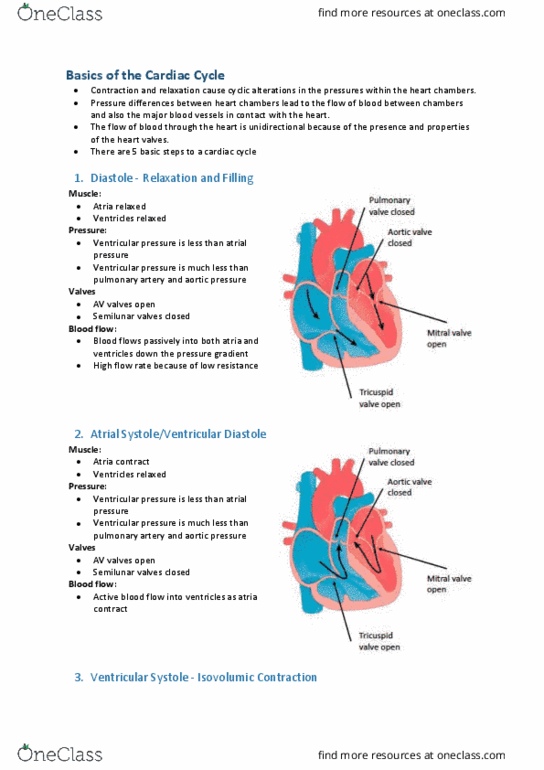
Pressure and Volume in LV
1. Mitral valve closes
• Isovolumic contraction
• Aortic valve still closed
2. Aortic valve opens
• Ejection: rapid at first then slows down as pressure in aorta increases
3. Aortic valve closes
• Isovolumic relaxation
• Mitral valve still closed
4. Mitral valve opens
• Passive ventricular filling - rapid at first then slows down
• Atrial contraction: active filling
Pressure Volume (LOOP) in LV
find more resources at oneclass.com
find more resources at oneclass.com

• Ends systolic pressure volume relationship (ESPVR)
• Describes the maximum pressure that can be generated for any given LV volume in a
fully contracted ventricle
• This slope is really a measure of contractility
• The steeper the slope the greater the inotropic state and the more pressure that can be
generated
find more resources at oneclass.com
find more resources at oneclass.com

• End diastolic pressure (EDPVR)
• Describes the pressure for any given amount of volume in a fully relaxed ventricle
• This slope is really the inverse of compliance (stretching of ventricle to accommodate
blood volume)
• The steeper the slope the less compliant the ventricle (its stiffer)
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Pressure and volume in lv: mitral valve closes. Isovolumic contraction: aortic valve still closed, aortic valve opens, ejection: rapid at first then slows down as pressure in aorta increases, aortic valve closes. Isovolumic relaxation: mitral valve still closed, mitral valve opens, passive ventricular filling - rapid at first then slows down, atrial contraction: active filling. What happens if venous return increases: an increase in venous return increases end diastolic volume (preload) of lv, esv and edv pressures are barely affected. Increased preload results in increased sv via frank-starling mechansim: this is o(cid:374)ly if (cid:271)oth afterload a(cid:374)d (cid:272)o(cid:374)tra(cid:272)tility are u(cid:374)(cid:272)ha(cid:374)ged (cid:449)hi(cid:272)h does(cid:374)"t ge(cid:374)erally happen in reality. What happens if aortic pressure changes: a decrease in aortic pressure will decrease afterload, a decreased afterload will result in increased sv. Increase in contractility (positive inotropy) increases slope of espvr: any given ventricular volume, the ventricle can generate more pressure. Increased sv: decrease in contractility will reduce slope of espvr and reduces stroke volume.