PHTY206 Lecture Notes - Lecture 19: Paresthesia, Long Bone, Traction Splint


Principles of fracture assessment and management
• A fracture is a break in the structural continuity of bone.
• The break may not be complete. Fractures include cracks, crumpling or splintering of part or all
of the bone
• Physiotherapy intervention in early management of fractures is largely directed at:
o Doing no further harm to the fracture site, while
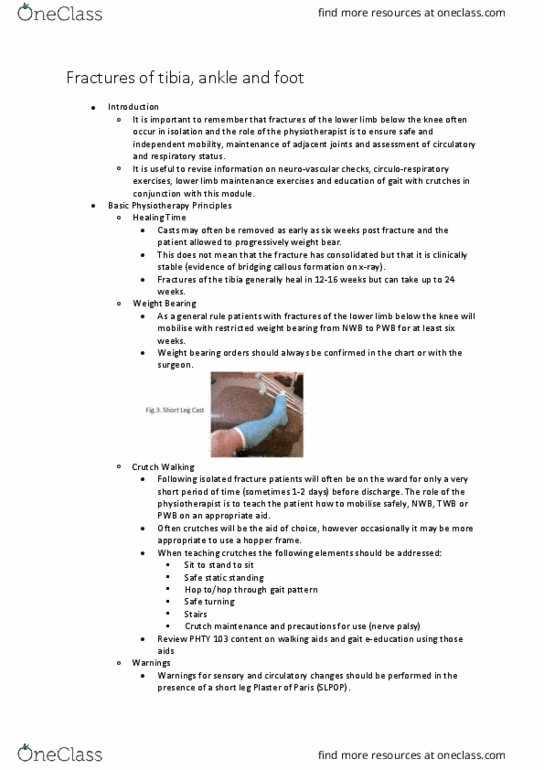
o Maintaining the integrity of the surrounding musculoskeletal, circulatory, neural and
respiratory systems and
o Facilitating safe and independent return to function
• Fracture healing is divided into stages for convenience and ease of classification. The stages
are not discrete and vary between individuals and fracture types.
• The 5 Stages of Fracture Healing are:
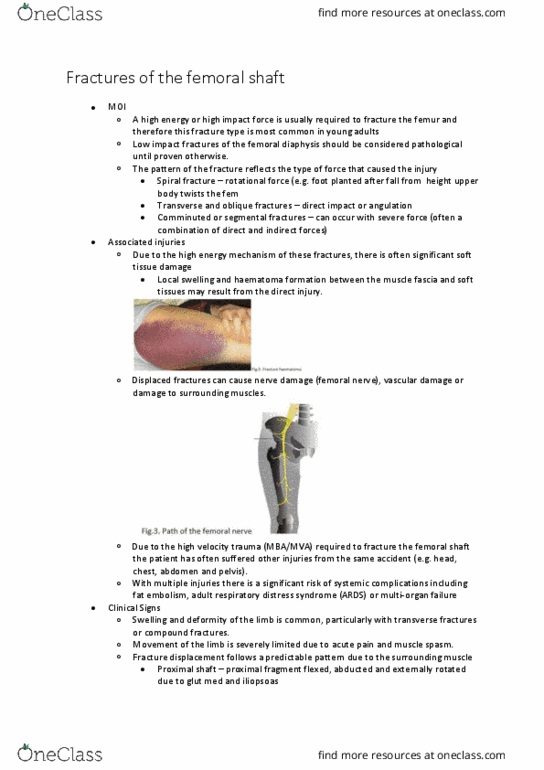
o Tissue destruction and haematoma formation
• Haematoma formation is the immediate result of the fracture
• Blood vessels are damaged and bleeding occurs between the ends of the fractured
bone
• An area of avascular necrotic bone results.
• The size of the haematoma influences the rate of healing with a small haematoma
delaying healing.
• The size of the haematoma depends on:
• The extent of periosteal disruption
• The extent of soft tissue damage
• The type of fracture
o Transverse fracture = small haematoma
o Spiral fracture = larger haematoma
o Inflammation and cellular proliferation (up to 2 weeks)
• Within 8 hours of the fracture occurring there is an acute inflammatory reaction
with proliferation of osteogenic cells from the endosteum and periosteum.
• Osteoclasts remove the necrotic bone and osteoblasts begin to lay down a matrix
of collagen which bridges the fracture site providing a scaffolding on which new
bone can be laid and in which new bone formation can take place.
• The clotted haematoma is slowly absorbed and fine new capillaries grow into the
area
o Callus (woven bone) formation (2-4 weeks)
• Callus formation starts at approximately 2 weeks
• The main bolus of callus is formed at about 4 weeks by which time the fracture
may be said to be 'united'.
• Thereafter callus does not increase in size but it does undergo substantial
reorganisation and gradually increases in stability.
• In this stage the proliferating cells can potentially form both bone and cartilage
given the right circumstances.
• The matrix of collagen formed by the osteoblasts between the periosteal and
endosteal surfaces becomes impregnated with calcium salts and develops into
woven bone
• As it becomes more densely mineralised movement at the fracture site decreases.
o Consolidation (4 weeks - several months)
• The transformation of callus (woven bone) into lamellar bone. In this stage
osteoclasts now migrate through the debris at the fracture line and resorb the
callus
• Osteoblasts lay down new bone in the gaps behind them.
find more resources at oneclass.com
find more resources at oneclass.com

• This is a slow process and lasts between four weeks and several months.
• Occurs earlier in the upper limb than the lower limb.
• Complete when the fracture appears clinically and radiographically united
• At this stage, there is no tenderness or movement at the fracture site
(clinical signs of union) and there is no evidence of a fracture line
(radiographic sign of union).
o Remodelling (2 months - 2 years post fracture)
• Remodelling is a continuous process of bone resorption and formation which
occurs at a relatively rapid rate for 1-2 years after a fracture.
• Thicker lamellae are laid down where the stresses are high, unwanted bone is
resorbed and the medullary canal is reformed as the bone approximates its
normal shape.
• Role of the Orthopaedic Physiotherapist in:
o Stage 1 and 2 of Fracture Healing
• To promote relative rest and oedema management in the form of immobilisation,
elevation and application of ice.
• To encourage circulo-respiratory and musculoskeletal maintenance exercises
where appropriate.
• To instruct patients on the use of appropriate mobility aids once fractures have
been immobilised either conservatively or surgically.
• To assess for circulatory or neurological impairment.
• To proide eduatio regardig the patiets ijur ad rehailitatio.
• Do no further harm (avoid activities that could delay or prevent fracture healing).
o Stage 3
• To encourage circulo-respiratory and musculoskeletal maintenance exercises
where appropriate.
• To instruct patients on the use of appropriate mobility aids once fractures have
been immobilised either surgically or conservatively.
• Do no further harm.
o Stage 4
• To instruct patients on the use of appropriate mobility aids once fractures have
been immobilised either surgically or conservatively.
• To progress weight bearing status, gait re-training, balance and strengthening
under the guidance of the orthopaedic doctor.
• Increase ROM of effected joints.
• Do no further harm.
• Once there is clinical union (i.e. no movement at the fracture site) a cast is often
removed and movement of previously immobilised joints adjacent to the fracture
site can be commenced (active/active assisted). The doctor’s decision to remove a
cast will most often be made after consulting a recent x-ray to confirm radiological
union.
• Predictors of fracture healing
o Simple rules for timeframes in fracture healing have been developed however they are
variable, e.g.
• Spiral fractures in the upper limb in children take 3 weeks to uni
• Spiral fractures in the upper limb in adults take 6 weeks to unite
• Spiral fractures in the lower limb take twice as long to unite (12 weeks)
• Transverse fractures take twice as long again
• For a fractured femur add 25%
o Therefore, using this simple rule it will take approximately 12 weeks for a transverse
fracture of the ulna to unite and 24 weeks for a transverse fracture of the tibia to unite.
find more resources at oneclass.com
find more resources at oneclass.com

o Other factors to consider include:
Factor to Consider
Effect
Age
The young heal faster
Site and type of fracture
Fractures at a site surrounded by muscle heal faster;
cancellous bone heals faster than cortical bone; oblique
and spiral fractures heal faster than transverse;
undisplaced fractures heal faster than displaced
Blood Supply to fragment
Scaphoid and head of femur fractures often result in
delayed union or sometimes avascular necrosis.
Mobility of fracture site
Excessive mobility slows healing but micro motion and
gentle weight bearing speeds healing.
Separation of bone ends
Can be caused by soft tissue interposition, excessive
traction, internal/external fixation
Infection
Slows healing
Joint Involvement
Slows healing
Bone Pathology,
Osteoporosis or bony
metastases
Delays Healing
As the rate of fracture healing can vary, it is important to be aware that some form of
support is required until clinical union of the fracture occurs.
• Classification of Fractures
o There are four main approaches to classifying fractures:
• Description and anatomical location
• Alphanumerical
• Mechanism of injury and
• Traditional (named after the originator)
o The classification of fractures according to description and anatomical location is
simplified through use of a step wise approach.
o 1. Skin Damage
• Open (compound) – direct communication between the broken bone and the skin
surface
• Closed (simple)- overlying tissues intact
find more resources at oneclass.com
find more resources at oneclass.com
Document Summary
Principles of fracture assessment and management: a fracture is a break in the structural continuity of bone, the break may not be complete. Fracture healing is divided into stages for convenience and ease of classification. Spiral fractures in the upper limb in adults take 6 weeks to unite. Spiral fractures in the lower limb take twice as long to unite (12 weeks: transverse fractures take twice as long again. Fractures at a site surrounded by muscle heal faster; cancellous bone heals faster than cortical bone; oblique and spiral fractures heal faster than transverse; undisplaced fractures heal faster than displaced. Scaphoid and head of femur fractures often result in delayed union or sometimes avascular necrosis. Excessive mobility slows healing but micro motion and gentle weight bearing speeds healing. Can be caused by soft tissue interposition, excessive traction, internal/external fixation. Skin damage: open (compound) direct communication between the broken bone and the skin surface, closed (simple)- overlying tissues intact, 2.