EAST 501 Lecture Notes - Lecture 10: Pancreatic Neuroendocrine Tumor, Neuroendocrine Tumor, Parathyroid Gland

21 Jun 2018
School
Department
Course
Professor
L8 – Gauthier Mar 14
Endocrine Tumors Part 1
1
CANCER IS A MAJOR KILLER
- ~1 in 2 Canadians expected to develop cancer during their lifetime
- About 50% of new cancer cases are (these are the 4 predominant cancers)
o Lung
o Breast
o Colorectal
o Prostate
WHAT ARE ENDOCRINE TUMORS?
- Endocrine tumors arise from parts of the body responsible for producing/secreting hormones
o Can be either hormone-secreting or not
§ over secretion of hormones can have deleterious effects
§ functional tumors = producing hormones à over-secretion can have deleterious effects
o Most are benign (adenomas), but can be metastatic
§ the cancerous tumors are carcinomas
- Main types of endocrine tumors are:
o Adrenal tumor
o Parathyroid tumor
o Pituitary gland tumor
o Neuroendocrine tumor
§ Carcinoid tumor – arise in the gut
§ Pancreatic neuroendocrine tumor
o Thyroid tumor
OUTLINE
1. Parathyroid tumors
2. Pituitary gland tumors
3. Neuroendocrine tumors
PARATHYROID HORMONE IS ESSENTIAL FOR CALCIUM HOMEOSTASIS
- Parathyroid glands secrete parathyroid hormone (PTH)
- 4 parathyroid glands at the back of the thyroid gland
- Calcium-sensing receptors on the parathyroid glands that sense/regulate Ca levels in the body
- PTH stimulates:
o Calcium release from bone (increased osteoclast activity)
o Calcium retention in kidney
o Formation of active vitamin D à calcium absorption in intestine
- when the serum Ca in low (detected by parathyroid glands) à increase in PTH (enters circulation and has
multiple sites of action)) à acts at multiple sites à PTH normalizes Ca by acting at different levels
o in the kidney PTH regulates Ca excretion, increases the production of Vitamin D (involved in the
retention of Ca in the gut)
o PTH acts on osteoclasts in the bone (osteoclasts = destroy bone and therefore release Ca)

L8 – Gauthier Mar 14
Endocrine Tumors Part 1
2
PARATHYROID ADENOMA (non-cancers/benign tumors) IS THE MAIN CAUSE OF PRIMARY HYPERPARATHYROIDISM
- 80-85% of primary hyperparathyroidism (PHT) caused by single adenoma (benign tumor = non-cancers)
o 2-5% caused by double adenoma; 10-15% caused by hyperplasia; <1% caused by carcinoma (potential to
metastasize or has already)
o single adenoma = only one gland is affected
§ adenomas are not that threatening
o primary hyperparathyroidism = when you have too high PTH in circulation caused usually by single
adenomas where only one gland is affected
§ sometimes you can have more than one tumor in the parathyroid gland
§ you can have simple hyperplasias where it is not a tumor yet
- PTH: common endocrine disorder, ~100 cases/100,000 individuals – not that uncommon
o Higher incidence in females (~3:1 ratio) – the biological reason for this is unknown
- Hyperparathyroidism characterized by inappropriately high PTH production
o Increased renal calcium retention
o Increase vitamin D production
o Increased bone resorption (more bone broken down and more Ca released)
o End result: hypercalcemia = too much Ca in the blood (life threatening)
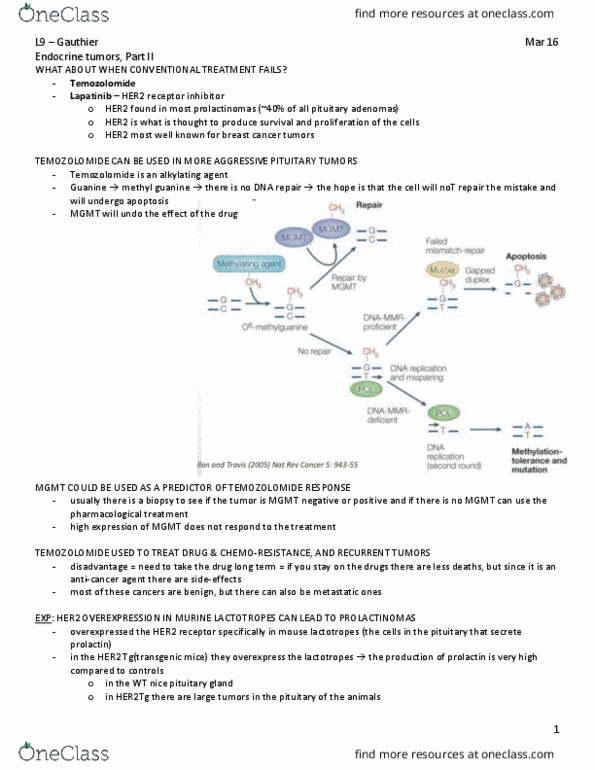
HYPERCALCEMIA IS USUALLY MORE LIFE-THREATENING THAN
THE CANCER ITSELF
- decreased water retention in the kidney = polyuria =
peeing more, less fluid in the body = further increase Ca concentration
- in the kidney if there is more Na = less water reabsorption

L8 – Gauthier Mar 14
Endocrine Tumors Part 1
3
- the figure above shows the renal physiology in the ascending limb of the Loop of Henle:
o Na/K/Cl symporter involved in the retention of 1 Na, 1K and 2Cl
o there is passive diffusion of K ions back into the tubule
o when you have hypercalcemia = increased Ca within the tubule = prevents the back diffusion of K ions =
pump inhibited (not enough K ions to drive the pump) à more Na in the tubule à less water
reabsorption à polyuria à decreased water reabsorption
- the most pressing issue with this type of tumor is controlling the Ca levels à can get out of hand very rapidly
- too much calcium:
o Mild symptoms: bone pain, vomiting
o Severe symptoms: coma, cardiac arrest, psychiatric side effects (delusions)
- the Ca levels MUST be corrected before even worrying about the actual tumor
TREATMENTS OF HYPERCALCEMIA CONSISTS OF FOUR GOALS
1. Correct dehydration
2. Enhance renal calcium clearance
o you want to excrete as much Ca as you can
3. Inhibit bone resorption
o inhibit the Ca loss from bone
4. Treat underlying disorder
o i.e. removing the tumor
IMMEDIATE COURSE OF ACTION SHOULD BE UNDERTAKEN TO CONTROL HYPERCALCEMIA
1. IV administration of isotonic fluid
o Restores intravascular volume
o Increases renal clearance
o Complications: fluid overload (especially in older patients), especially in cases of heart failure
o sometimes need to give as much as liters of fluid
o this is a very effective first step (immediate first step)
o decreases Ca concentration in the blood
2. Loop diuretics (furosemide or ethacrynic acid) – stimulate kidney function = excretion of more urine and Ca
o these drugs inhibit Na-K-Cl symporter + inhibits calcium re-absorption
o Protects against fluid overload (older/cardiac patients)
o Complications: loss of other electrolytes (or too many electrolytes)
§ this is why it is not used as much, compared to fluid admin, accept in older patients
o usually reserved for elderly patients
o 9mg/dL is ~ the normal range for Ca
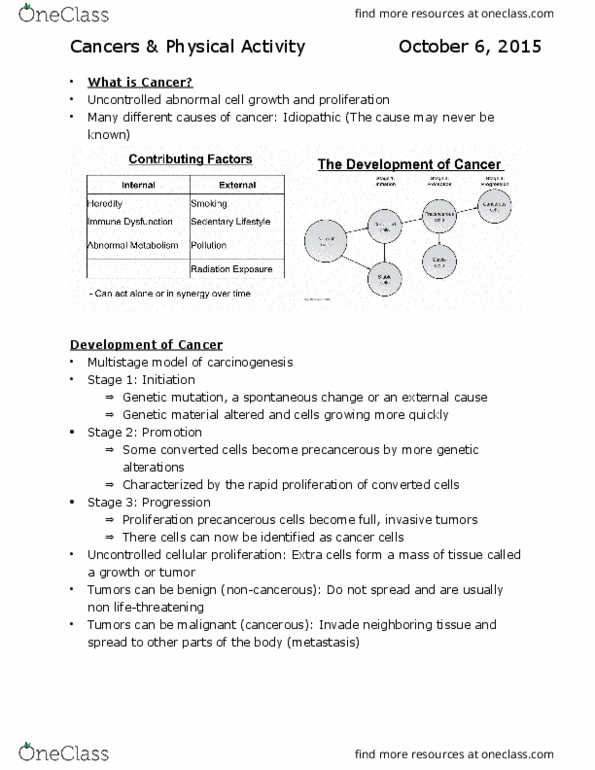
A QUICK SNAPSHOR OF BONE METABOLISM
- the production of RANKL by
osteoblasts is required for
osteoclast function
Document Summary
~1 in 2 canadians expected to develop cancer during their lifetime. About 50% of new cancer cases are (these are the 4 predominant cancers: lung, breast. Endocrine tumors arise from parts of the body responsible for producing/secreting hormones: can be either hormone-secreting or not. Over secretion of hormones can have deleterious effects functional tumors = producing hormones over-secretion can have deleterious effects: most are benign (adenomas), but can be metastatic the cancerous tumors are carcinomas. Main types of endocrine tumors are: adrenal tumor, parathyroid tumor, pituitary gland tumor, neuroendocrine tumor. Carcinoid tumor arise in the gut. Outline: parathyroid tumors, pituitary gland tumors, neuroendocrine tumors. 4 parathyroid glands at the back of the thyroid gland. Calcium-sensing receptors on the parathyroid glands that sense/regulate ca levels in the body. Pth stimulates: calcium release from bone (increased osteoclast activity, calcium retention in kidney, formation of active vitamin d calcium absorption in intestine. Parathyroid adenoma (non-cancers/benign tumors) is the main cause of primary hyperparathyroidism.