PATH 300 Lecture Notes - Lecture 9: Breast Cancer, Adipose Tissue, Bronchus

26 Apr 2019
School
Department
Course
Professor

PATH300
Breast and prostate cancer
Statistics
-same across North America for 2017 :
prostate and breast cancer are about 1/8
lifetime probability ; most people will be
successfully treated
-lung and bronchus : incidence and death are
very close ; breast and cancer : most people
survive
-risk factors : environment (5% cases is
genetic, same one for breast and cancer)
-both have links to obesity in terms of
risk factors -> obesity increases very
rapidly in all developed countries =>
risk factor for many other diseases
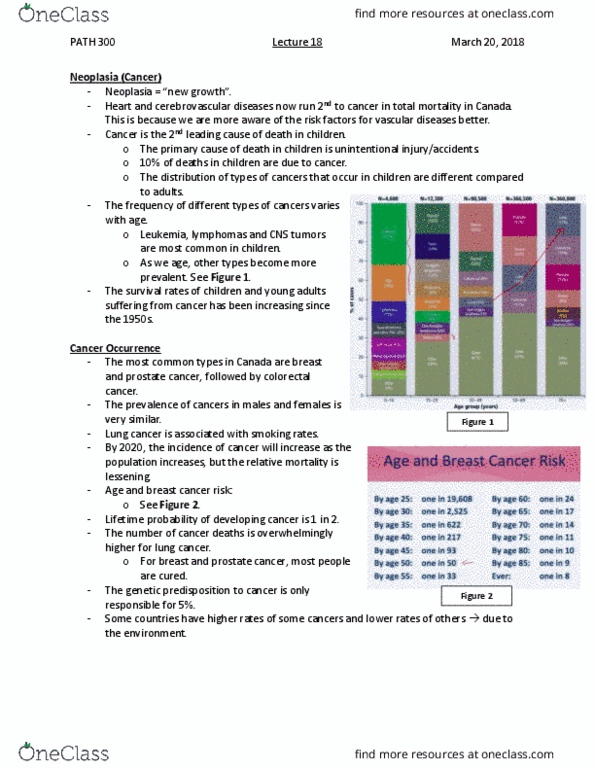
-prevalence increases with age, not many
situations before around 40 ; mortality goes up with age as well
-death rate : ~13-14%, becomes even better for prostate cancer (now less than 10%)
-incidence and death rate : not the same in all places, detect early = lower death rate
Parallels between breast and prostate cancer
-incidence #1 and mortality #2
-both hormone related -> both respond to hormone therapy
-both metastasise to bone, liver and lung
-both sensitive to chemotherapy and radiation
-mainly asymptomatic
-surgical treatment used to be radical, now conservative
-for both of these, metastasis can occur fairly late in the progression of the disease -> keep an eye
on the patients for about 10 years after treatment (5 years for other cancers)
-epidemiology similar, with similar lifestyle risk factors
-age and survival rates are similar
Breast cancer
-survival rate is very high (except for very advanced age)
-risk is age related : we have to know how those statistics are compiled : risk for
breast cancer depends on the age ; when we compare the incidence between
countries, be careful of the age
-many of us will live over 90, and we expect much greater understanding => expect
risk of 1/8 to decrease
-tumor distorts lobule in the breast => dimpling in the surface of the skin,
sometimes people can feel the lump
-tumor cells can infiltrate the adjacent adipose tissue
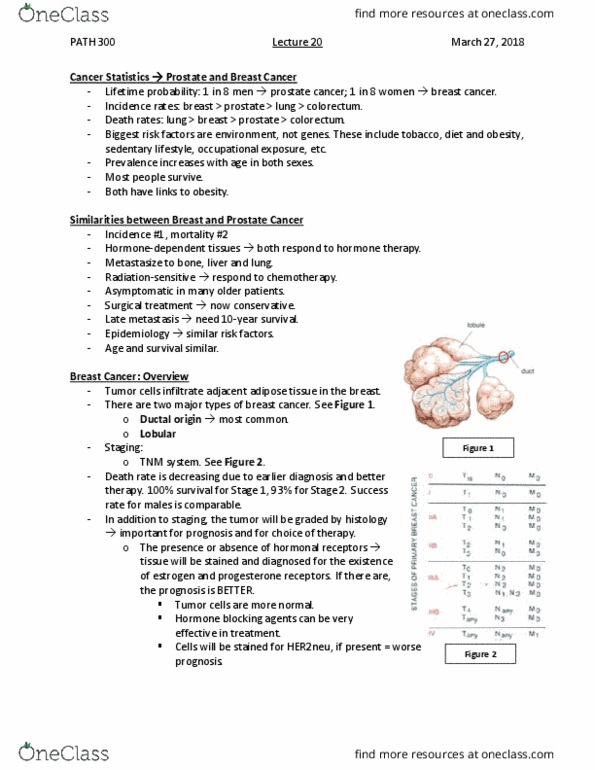
-depending on cells of origin, different types :
-ducts : most common ones ; tumor growing inside the duct -> if detected,
carcinoma in situ is always curable because no invasion => take out the lump of the breast
and the person will be fine
1

-invasive ductal carcinoma : walls of the ducts invaded => spread, we have to do tests to
find out where it may be
-lobules (milk glands) : in situ : in cells within lobules (if caught early enough, it can be
cured)
-invasive lobular carcinoma : grows in surrounding adipose tissue
Staging
-size of the tumor determined by different types of scans… ; lymph nodes
invasion and how many ; distant metastasis
-early : if detected with mammography or other methods -> get rid of it and
we are cured
-if not in situ -> look at the size of the primary tumor, spread of the tumor to
regional lymph nodes (most common is to lymph nodes on the sides of the
breast and under the arms) -> estimate without surgery is possible
-metastasis : lung, liver and bones => fatal and painful
-T 1-4 ; N1-3 ; M positive or negative => combine the scale and look up on
the chart and see where the person will be categorised
Trends in cancer death rate among females
-death rate is going down (since fairly recently) -> in
contrast to liver cancer for example which has been going
up
-survival rate has been improving because of earlier
diagnosis and better therapy (mammograms done
periodically after certain age in certain countries…)
-stage 1 : 100% survival, stage 2 : 93% survival, stage 3 :
72% ; stage 4 : still better than pancreatic cancer
-when we look at 5 years survival -> monitor people that
were diagnosed more than 5 years ago -> lot of optimism
-men can get breast cancer too (if they take female
hormones, breast can develop) ; success rate for treatment is
the same
-stage at diagnosis is earlier now (1 and 2 in the great majority of patients)
Grading of the tumor
-always done
-earlier stage tumor with negative looking grade will be of more risk than otherwise
-look at structure, characteristics and staining properties of the histological section of the tumor
-receptors present on their surface, features, cell divisions (proliferation index = how quickly
they are dividing), structure of the cells… => grade is an important feature in prognosis and in
which method of therapy to use
-look for presence / absence of hormonal receptor : tissue will be stained and diagnosed
(estrogen and progesterone receptors) -> if present, prognosis is better (tumor cells are thus
more normal, hormone blocking agents can be very effective in treating these tumors)
-HER2 : cells will be stained for this, if highly present -> worst prognosis (but therapy which is
temporarily effective)
Looking at tumors
-primary tumor thanks to immunochemistry
-look at collecting lymphatics, at the sentinel lymph node (primary drains the area of the breast
where the primary tumor is located)
2

-look at cancer markers in the blood
-prognostic features in addition to staging :
-look at histological grading -> number depends on the abnormality level of the tumor
(higher the grade, worst the prognosis, the more abnormal the cells look like)
-vascular invasion (tumor will be classified with hormone receptor status and response -> if
tumor is positive, very positive way to treat it)
-HER2 status (growth factor receptor) : over expressed, associated with poor prognosis but
monoclonal antibody developed against this particular receptor -> can be very effective
temporarily in relief of this type of cancer
-more lymph nodes involved -> larger the size of the tumor
3
Document Summary
Same across north america for 2017 : prostate and breast cancer are about 1/8 lifetime probability ; most people will be successfully treated. Lung and bronchus : incidence and death are very close ; breast and cancer : most people survive. Risk factors : environment (5% cases is genetic, same one for breast and cancer) Both have links to obesity in terms of risk factors -> obesity increases very rapidly in all developed countries => risk factor for many other diseases. Prevalence increases with age, not many situations before around 40 ; mortality goes up with age as well. Death rate : ~13-14%, becomes even better for prostate cancer (now less than 10%) Incidence and death rate : not the same in all places, detect early = lower death rate. Both hormone related -> both respond to hormone therapy. Both metastasise to bone, liver and lung. Surgical treatment used to be radical, now conservative.