PSYC 212 Lecture Notes - Lecture 18: Receptive Field, Mechanoreceptor, Proprioception

6 Nov 2018
School
Department
Course
Professor

Touch
What is touch?
Terminology
Somatosensation: collectively, sensory signals from the skin,
muscles, tendons, joints, and internal receptors
§
Kinestheisa: perception of the position and movement of our limbs
in space
§
Proprioception: perception mediated by kinesthetic and internal
receptors (e.g. stomach)
§
○
Note: the use of these terms can vary considerably from one author to
another
○
•
Touch physiology
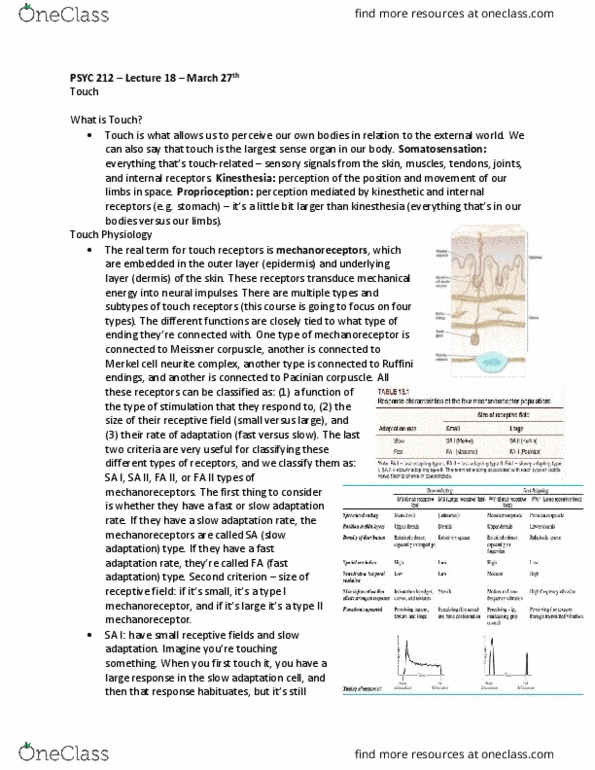
Touch receptors: embedded in outer layer (epidermis) and underlying
layer (dermis) of skin
Multiple types of touch receptors
§
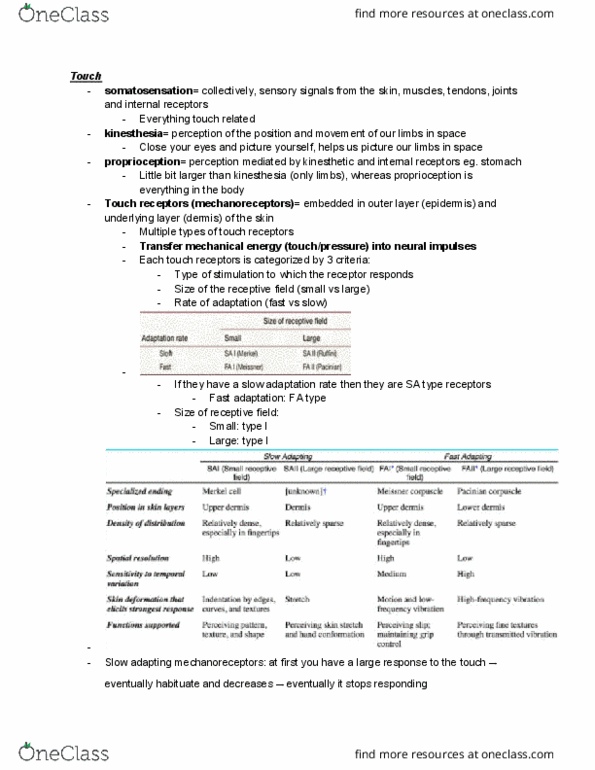
Each touch receptor can be categorized by three criteria
§
Types of stimulation to which the receptor responds
1.
Size of the receptor field
2.
Rate of adaptation (fast vs slow)
3.
○
Spatial event plot of a SA1 fiber
In the first pass, when the bottom edge of the bottom dot in the
Braille pattern just crosses the top of the receptive field, the fiber
responds with a single action potential
§
By the third pass, the whole top dot is sweeping across the middle
of the receptive field, and the fiber responds with a burst of four
action potentials
§
In the seventh pass, the three center dots are crossing the middle
of the receptive field, and the three bursts are correspondingly
more robust
§
○
Tactile receptors (mechanoreceptors)
Feeling the shape of your key in your pocket requires the SA1 (and
maybe also the FA1) channel
§
Shaping your fingers to grasp the key involves the SA2 channel
§
As you insert the key into the lock, your grip force increases so that
the key does not slip, thanks to your FA1 channel
§
Finally, your FA2 channel tells you when the key has hit the end of
the keyhole
§
○
•
Proprioception
Strange case of neurological patient Ian Waterman
Cutaneous nerves connecting Waterman's kinesthetic and tactile
mechanoreceptors to brain destroyed by infection
§
Lacks kinesthetic senses, dependent on vision to tell limb positions
§
Still had pain and temperature sensation
§
Every time he wanted to move or talk, he'd have to think about it
Actions were no longer automatic□
§
○
•
Touch physiology
All touch fibers eventually bundle up together into a nerve that enters the
spinal cord between each vertebral disc
○
Each area of the skin innervated by a specific nerve is called a dermatome
○
How finely can we resolve spatial details?
Two-point threshold: the minimum distance at which two stimuli
are just perceptible as separate
§
Like sensitive to pressure, spatial acuity varies across the body
Extremities (fingertips, face, and toes) show the highest
acuity
□
§
○
Dorsal column-medial lemniscal (DCML) pathway: carries signals from
skin, muscles, tendons, and joints
Most fibers project directly to the gracile and cuneate nuclei
§
Ascending inputs remain ipsilateral until they cross at the level of
the pyramids in the medulla
§
After a second synapse in the thalamus, fibers reach the
somatosensory cortex
§
○
Touch sensations are represented somatotopically in the brain
Primary somatosensory cortex called S1; secondary somatosensory
cortex called S2
§
Analogous to retinotopic mapping found in vision
§
Adjacent areas on skin connect to adjacent areas in brain
Homunculus: maplike representation of regions of the body
in the brain
□
§
○
Body image: the impression of our bodies in space
Our body images are systematically distorted towards top-
heaviness
Expanded shoulders and upper arms□
People rate upper half of body to be larger than lower half□
Consistent with somatotopic mapping in cortex and sensory
homunculus
□
§
○
Phantom limb: sensation perceived from a physical amputated limb of
the body
Parts of the brain listening to missing limbs not fully aware of
altered connections, so they attribute activity in these areas to
stimulation from missing limb
Body image is inaccurate□
§
Amputees report feeling the amputated hand when their face or
remaining limbs are stimulated
Face area is located next to hand and arm area on sensory
homunculus
□
Neural crosstalk leads to sensory crosstalk□
The face area of the brain notices that the part of the
arm/hand is now unused, so the face tries to take over that
area
Doesn't mean that the face becomes more sensitive
®
□
§
Phantom limb pain:
60-80% of patients have painful phantom sensations□
Phantom limb is almost completely absent in young infants□
5-10% of patients the pain is severe□
Pain appears in the first day/weeks following the amputation□
Pain is intermittent and tends to decline with time□
How to prevent the functional reorganization if the limb is
missing?
You have to fool the brain into thinking that the limb is
still there
®
Mirror therapy
Putting a mirror next to limb that is still there
(leg), so that the missing limb will appear to be
there in the mirror (other leg)
◊
®
Prosthesis use
Rarely report phantom limb pain
◊
®
□
§
○
•
Lecture 18(19/20)
Tuesday, March 27, 2018
12:57 PM