PSYC 337 Lecture Notes - Lecture 7: Generalized Anxiety Disorder, Panic Attack, Imipramine

7 May 2018
School
Department
Course
Professor

Lecture 7: Anxiety
●Freud would say that anxiety is the chief concern
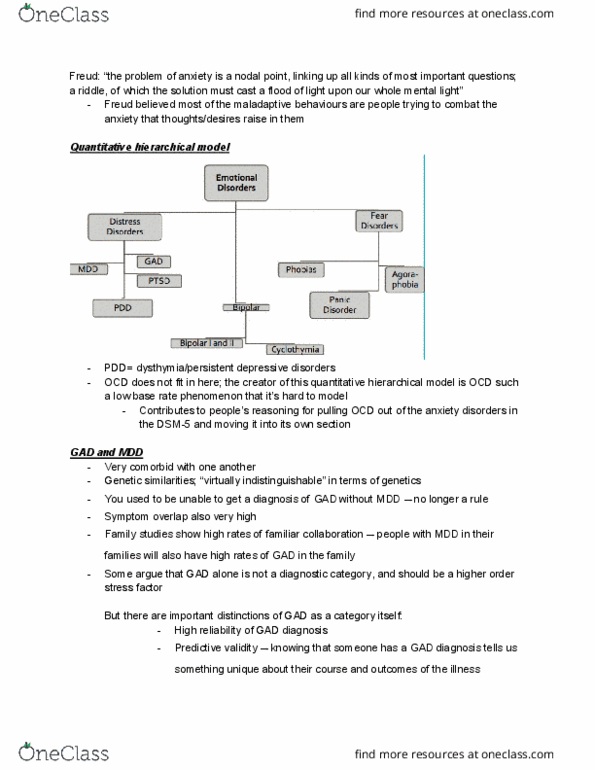
●Quantitative Hierarchical Model of internalizing/emotional disorders
○
■OCD is not included here, due to a low base rate phenomenon
●Generalized Anxiety Disorder (GAD)
○GAD and MDD
■Very comorbid; rare to meet someone with GAD who has never had a diagnosis
of a major depressive episode
■They have genetic similarities, with Watson arguing that they are virtually
indistinguishable
●High rates of familial coaggregation (people with MDD have lots of
family members with GAD, and vice versa)
■Used to be that you could not diagnose GAD if you only had it within a MDD
episode, not so anymore
■Symptom overlap is very high
■Some people say that GAD should not be its own thing, but it does have
important distinctions showing that GAD is a meaningful category in itself
●We have good reliability in GAD diagnosis
○Also high predictive validity (in terms of the course of their
illness and outcomes)
●Different mechanisms (e.g. attentional and memory biases, and
intolerance of uncertainty)

●Low positive affect (as a unique factor for depression, and not GAD - in
GAD they can have positive affect)
●Precipitation stressors
○Humiliation → MDD
○Danger events → GAD
●Different responses to lab stressors
○Blunting responses across the board in MDD
○Hyperreactivity to threatening stimuli in GAD
●Temporal course
○Trait anxiety tends to be predictive of GAD
○Some people suggest a linear movement from MDD to GAD
■Extreme goal focus of GAD moving to motivation
disengagement in MDD
■Moving from uncertainty that is intolerable in GAD to a
certainty of negativity in the future in MDD
■Beliefs about helplessness in GAD to beliefs of
hopelessness in MDD
○GAD is not a “prototypical” anxiety disorder (like phobias, panic disorder)
■Typically, in these other anxiety disorders there is a discrete focus of fear (e.g. a
phobic object like spiders, or panic attacks)
■People greatly fear these objects, and actively avoid them and related things
(generalized behavioural avoidance)
■In contrast, for GAD the fear object is the emotional experience or response to
threat (i.e. “bad” emotions)
●People catastrophize about the experience of anxiety
●E.g. passive genetic transmission of anxiety; Prof Weinberg was anxious
about grad school, and her father (who has trait anxiety) told her “if you
don’t stop being anxious you’ll die”; he has passed on both the genes for
trait anxiety AND a way of thinking about/catastrophizing about anxiety
■There is a persistent pattern of uncontrollable worry in GAD; typically you are
worrying about a multitude of things

●While everyone worries about family, school, work, etc., people with
GAD can’t control these thoughts and spend a much larger proportion of
time worrying
○GAD in the DSM-5
■DSM-II had lumped it into a broad category of “anxiety neurosis”, until in
DSM-III GAD became its own category (but it was a catch-all, nonspecific for
people who didn’t fit into proper other disorders)
●In DSM-II-R, GAD got its own identity and diagnostic criteria → this
was when worry bagn to play a larger role
○Important - it must be pathological worry about everyday
situations
○Difficult to diagnose, because many other disorders have worry
symptoms (MDD, phobias)...important for GAD is that there is
no one specific focus
■DSM-IV
●Simplified the criteria
○Excessive anxiety/worry
○More days than not, for at least 6 months
○About multiple events, activities, objects
○Difficult to control
○Cannot occur exclusively during a mood episode
■DSM-V criteria (if you meet above criteria, you need 3 of the below)
●Restlessness, feeling on edge
●Easily fatigued
●Difficulty concentrating
●Irritability
●Muscle tension
●Sleep disturbance
●Causing significant distress or impairment
■It’s a controversial disorder, because it is almost ALWAYS comorbid with
something else (so is it just a symptom of other things)
●It may be a vulnerability marker?
■Prevalence rates
Document Summary
Freud would say that anxiety is the chief concern. Ocd is not included here, due to a low base rate phenomenon. Very comorbid; rare to meet someone with gad who has never had a diagnosis of a major depressive episode. They have genetic similarities, with watson arguing that they are virtually indistinguishable. High rates of familial coaggregation (people with mdd have lots of family members with gad, and vice versa) Used to be that you could not diagnose gad if you only had it within a mdd episode, not so anymore. Some people say that gad should not be its own thing, but it does have important distinctions showing that gad is a meaningful category in itself. We have good reliability in gad diagnosis. Also high predictive validity (in terms of the course of their illness and outcomes) Different mechanisms (e. g. attentional and memory biases, and intolerance of uncertainty)